
Radioisotopic Evaluation Glomerular Filtration Rate (GFR) before and after Kidney Donation
Vincenzo Cantaluppi1, Gabriele Guglielmetti1, Marta Mora1, Federica Orsini2, Andrea Airoldi1, Marco Quaglia1, Gian Mauro Sacchetti2, Claudio Ronco3.
1Nephrology and Kidney Transplantation Unit, University of Piemonte Orientale (UPO), Novara, Italy; 2Nuclear Medicine Unit, Maggiore della Carità University Hospital, Novara, Italy; 3Nephrology, Dialysis and Kidney Transplantation Unit, International Renal Research Institute (IRRIV), Vicenza, Italy
Background: Because of the decrease of the nephron mass following nephrectomy, kidney donors (KD) develop a partial loss of renal function defined as Acute Kidney Injury (AKI) according to KDIGO criteria (Clinical Practice Guideline, 2012). The recovery of renal function following AKI is mainly ascribed to the concept of renal functional reserve (RFR), defined as the capacity of the kidney to increase glomerular filtration rate (GFR). However, only few studies correlated RFR in KD with long term functional outcomes.
Aim of the Study: The aim of the present study was to analyse 30 KD renal function before nephrectomy, in the immediate postoperative period and 1 year after the surgical procedure, developing the concept of estimated RFR (eRFR) for the long term follow-up of renal function in KD.
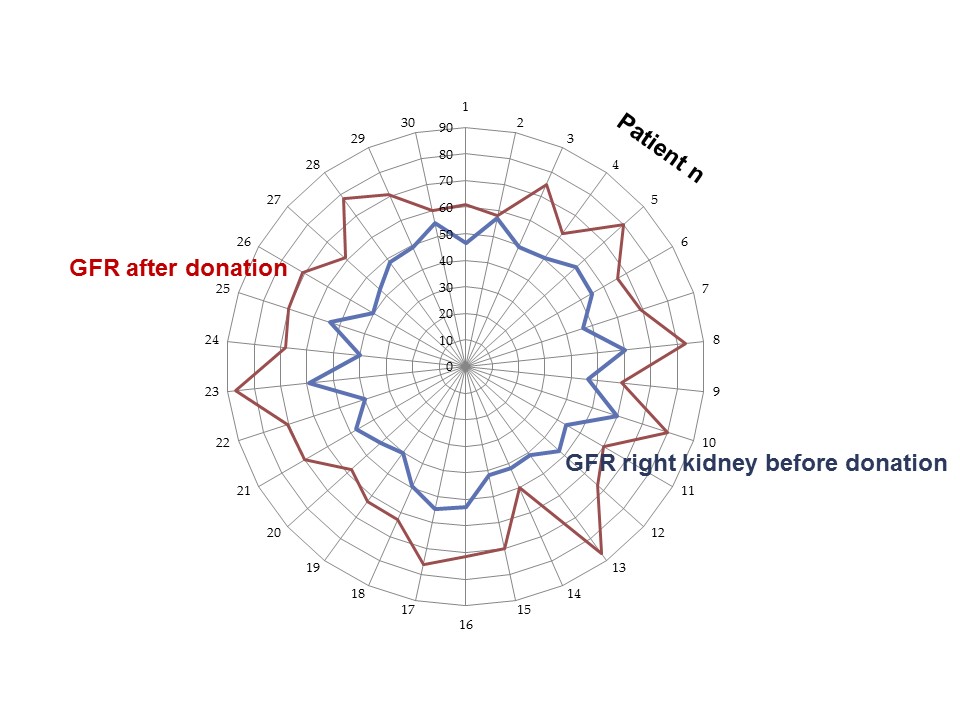
Results: KD mean age at the time of donation was 54.4 years (min-max, 30-78), mean serum creatinine 0.73 mg/dL (0.5-0.96), eGFR (CKD-EPI) 99 mL/min/1.73m2 (69-119) and radioisotope (51Cr-EDTA) GFR 101.4 mL/min (78-129). The split function was evaluated by concomitant scintigraphy using 99mTc-MAG: the mean percentage of renal function of right kidney was 48% (43-56) and left 52% (44-57), respectively. As expected, immediately after nephrectomy all KD worsened renal function: the mean percentage increase of serum creatinine was 79% (50-112.2%) within 72 hours post-surgery; most of KD (25/30) developed AKI stage 1, and 5 KD AKI stage 2 according to KDIGO criteria. Seven days after surgery, renal recovery was observed in all cases: the mean percentage increase of serum creatinine (50.6%) was significantly lower than the zenith of serum creatinine. These results suggest a potential gain of about 30% in comparison to the starting value of the right kidney. One year after nephrectomy (all KD were subjected to left nephrectomies), we studied KD renal function (GFR) by radioisotopic evaluation using 51Cr-EDTA and we then compared it with the split radioisotope (51Cr-EDTA) GFR of the right kidney at the first scintigraphic evaluation. Mean GFR was 68.8 mL/min (50-87) vs. 48.6 mL/min (39.7-60.4) before donation with an average GFR increase of 20 mL/min (0.8-45.6) and a percentage increase of the right renal function up to 110% (mean 42%, min 1.4%).
Conclusions: The results of this study show that radioisotopic evaluation is feasible and allows an estimated determination of RFR at different time points after nephrectomy in KD. We observed a compensatory hypertrophy due to RFR in all the 30 KD included in the study, independently from age and co-morbidities such as elevated BMI and hypertension. The limitation of this study is the evaluation of RFR only after the decrease of the nephron mass due to donation: we have now started a kidney stress test with a protein load to estimate RFR of KD before surgery with the aim of finding a correlation with radioisotpic GFR after nephrectomy.

