
High Risk Donor Kidneys should be Used in Pediatric Kidney Transplant Recipients
Malcolm MacConmara1, Ali El Mokdad1, Swee Levea2, Christine Hwang1.
1Surgery, University of Texas Southwestern Medical Center, Dallas, TX, United States; 2Medicine, University of Texas Southwestern Medical Center, Dallas, TX, United States
Introduction: There continues to be a shortage of kidneys for pediatric patients listed for transplantation. A strategy to increase the donor pool would be to utilize kidneys from donors who are considered to be Centers for Disease Control and Prevention (CDC) high risk for transmission of certain types of infections. We questioned if use of CDC high risk kidneys in the pediatric patient population was warrented by examining outcomes in this patient population.
Materials and Methods: The United Network for Organ Sharing database was examined to investigate outcomes in all kidney transplant recipients from 1996 to 2017. The patients were then divided upon adult and pediatric (under age 18 years) status and presence or absence of CDC high risk status. Donor and recipient demographic data were examined, and Kaplan Meier survival curves were generated. Categorical differences were compared using the unpaired Student's t-test and nominal variables using either the Chi Square or Fischer's exact test. A p-value of <0.05 was considered to be significant.
Results and Discussion: A total of 357 pediatric kidney transplant recipients received a kidney from a CDC high risk donor. The average donor age in the pediatric CDC high risk recipient group was 22.0 vs. 28.6 years (p<0.05) in the non CDC high risk recipients, and the average KDPI in the CDC high risk group was 18% vs. 24% (p<0.05). The average cold storage time in the CDC high risk group was 14.3 vs. 10.3 hours (p<0.05). The average age in the CDC high risk recipients was 11.3 vs. 10.7 years (p<0.05), and the length of stay was 13.0 vs. 13.2 days (p=NS) in the high risk vs. non high risk groups. The rate of rejection in the first year post transplant was significantly higher in the non CDC high risk group, 27.0% vs. 16.8% (p<0.05). When examining patient and allograft survival in all pediatric recipients who received a CDC high risk allograft, survival was not significantly different between the two groups.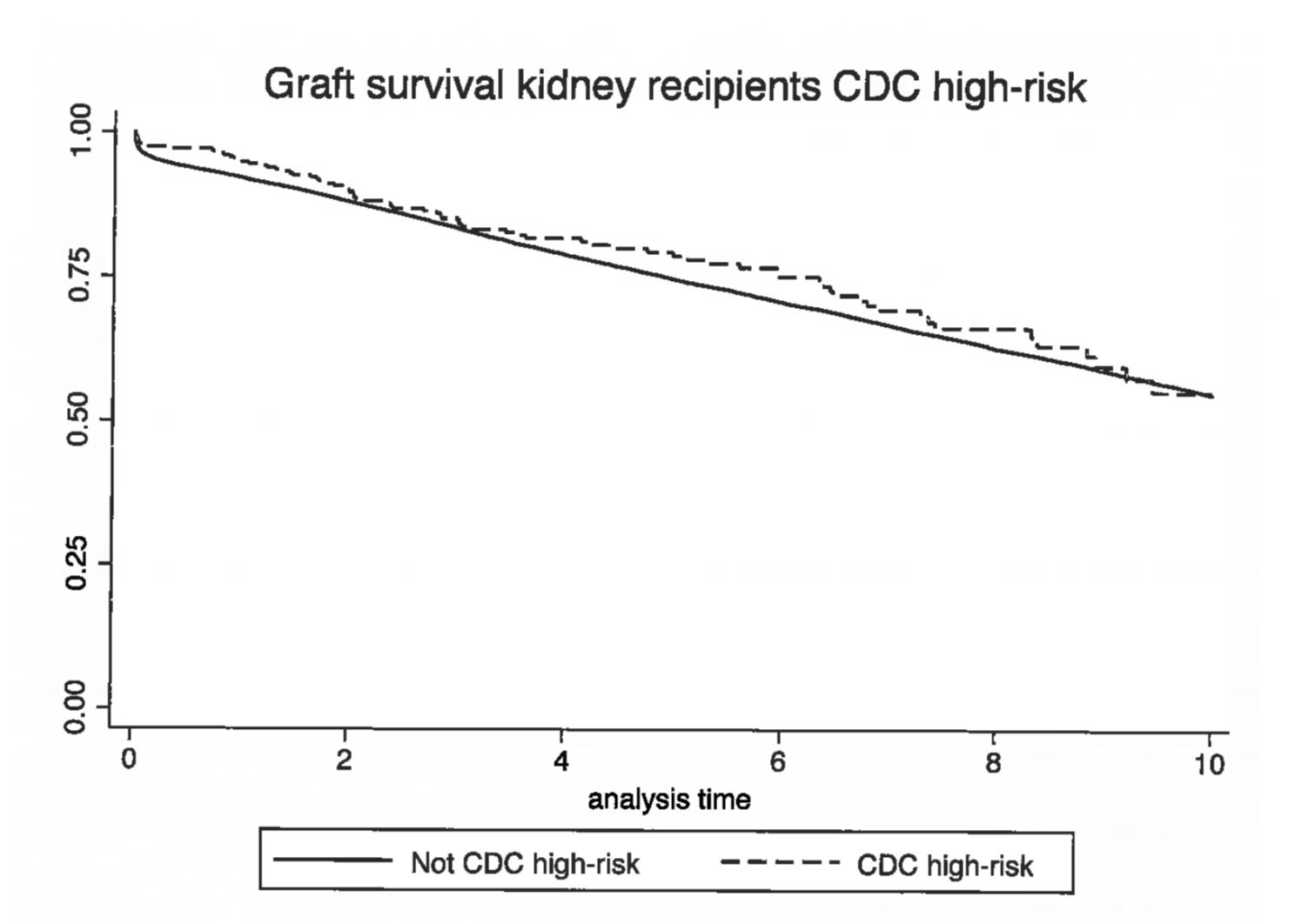
The donors in the CDC high risk group were significantly younger, had a lower KDPI, and had a longer cold storage time. The recipients in the CDC high risk were older, had fewer rejections, and had no significant difference in length of stay. Patient and allograft survival were similar when compared to those recipients who did not receive a CDC allograft, indicating that the CDC high risk kidney is a viable option to increase the donor pool for kidneys in pediatric recipients.
Conclusion: Patient and allograft survival in CDC high risk donor kidneys is similar to those allografts that are not considered to be CDC high risk. Use of CDC high risk kidney allografts should be strongly considered to increase the organ pool for pediatric patients.

