
Patrick B Trotter, United Kingdom has been granted the TTS Young Investigator Scientific Award
Transplantation of Kidneys from DCD and DBD Donors who Died after Ligature Asphyxiation: the UK Experience
Patrick Trotter1,2, Matthew Robb2, William Hulme2, Christopher Watson1, James Neuberger3, J A Bradley1.
1Department of Surgery , University of Cambridge, Cambridge, United Kingdom; 2Statistics and Clinical Studies, NHS Blood and Transplant, Bristol, United Kingdom; 3The Liver Unit, Queen Elizabeth Hospital, Birmingham, United Kingdom
Introduction: Kidneys from donors who die after ligature asphyxiation are often used for transplantation but there is concern that the hypoxic injury following ligature asphyxiation may be associated with inferior transplant outcomes, particularly when kidneys incur additional ischaemic injury during donation after circulatory death (DCD).
Materials and Methods: The UK transplant registry was used to identify all donors who died secondary to ligature asphyxiation from 1/1/2003-1/1/2017 through manual review of the free text entries in deceased organ donor forms. Survival analysis, cox proportional hazards regression and logistic regression models were used to determine the effect that both donation after brain stem death (DBD) and DCD donors who died after ligature asphyxiation had on renal transplant outcomes.
Results: Over the 14-year study period, 2.7% (n=521) of all potential UK organ donors died secondary to ligature asphyxiation. Nearly all were a result of attempted suicide by hanging (98.7%). Of this number 409 (78.5%) proceeded to donate kidneys for transplantation, of which 192 (46.9%) were DBD donors and 217 (53.1%) were DCD donors. Both DBD and DCD kidney donors who died from ligature asphyxiation were significantly younger, a greater proportion were male, and had markedly lower levels of hypertension and cardiac disease than donors who died from causes other than ligature asphyxiation. Donors who died following ligature asphyxiation provided kidneys for 650 kidney only transplants. 12-month eGFR was significantly better for those who received kidneys from donors who died from ligature asphyxiation (both DCD and DBD). 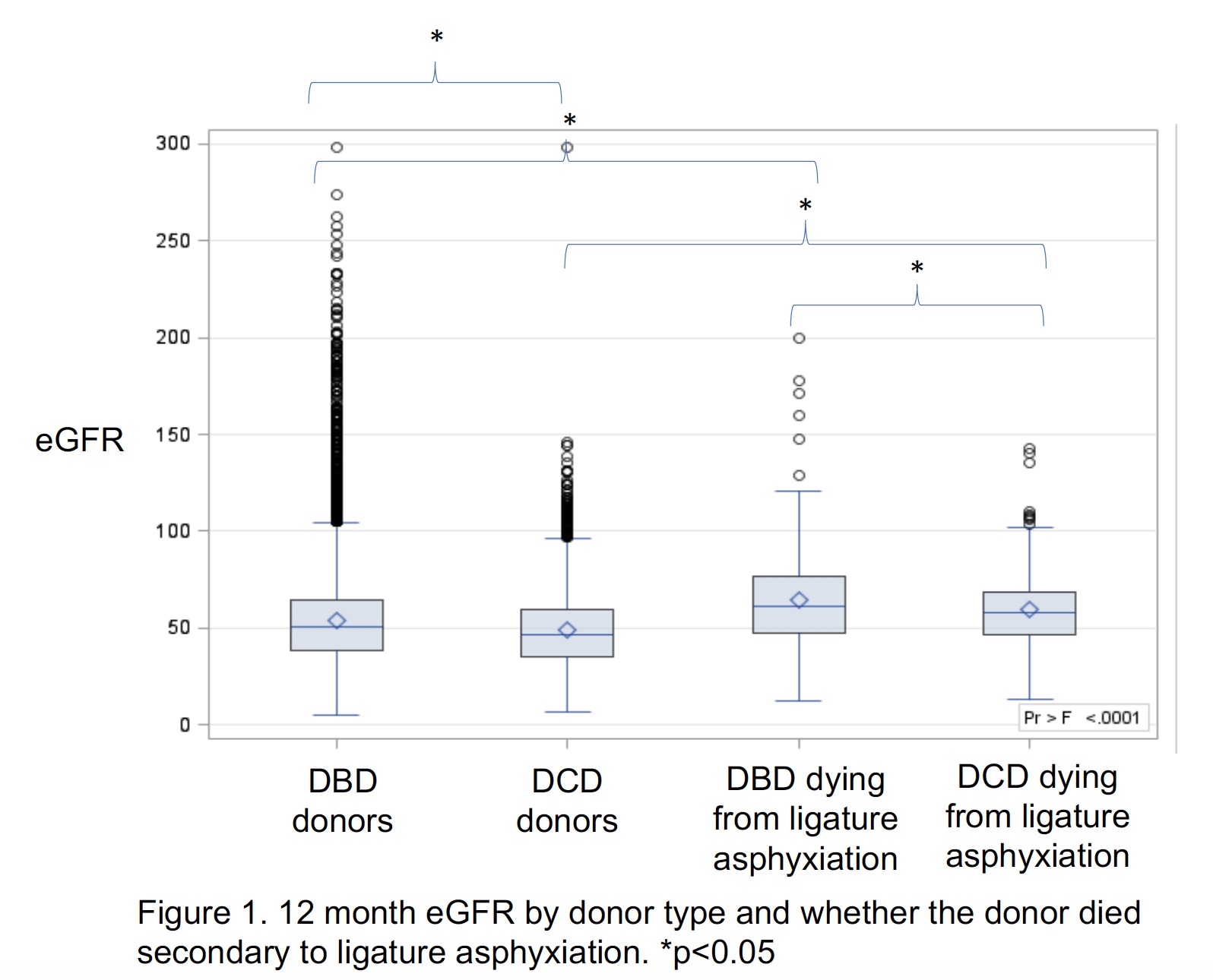 After adjustment for both donor and recipient factors using multivariate linear regression, receiving a kidney from a donor who died following ligature asphyxiation was not an independent predictor of better 12-month eGFR (p=0.625). Recipients of kidneys from donors who died following ligature asphyxiation (both DCD and DBD) had significantly better unadjusted 5-year patient and death censored graft survival.
After adjustment for both donor and recipient factors using multivariate linear regression, receiving a kidney from a donor who died following ligature asphyxiation was not an independent predictor of better 12-month eGFR (p=0.625). Recipients of kidneys from donors who died following ligature asphyxiation (both DCD and DBD) had significantly better unadjusted 5-year patient and death censored graft survival.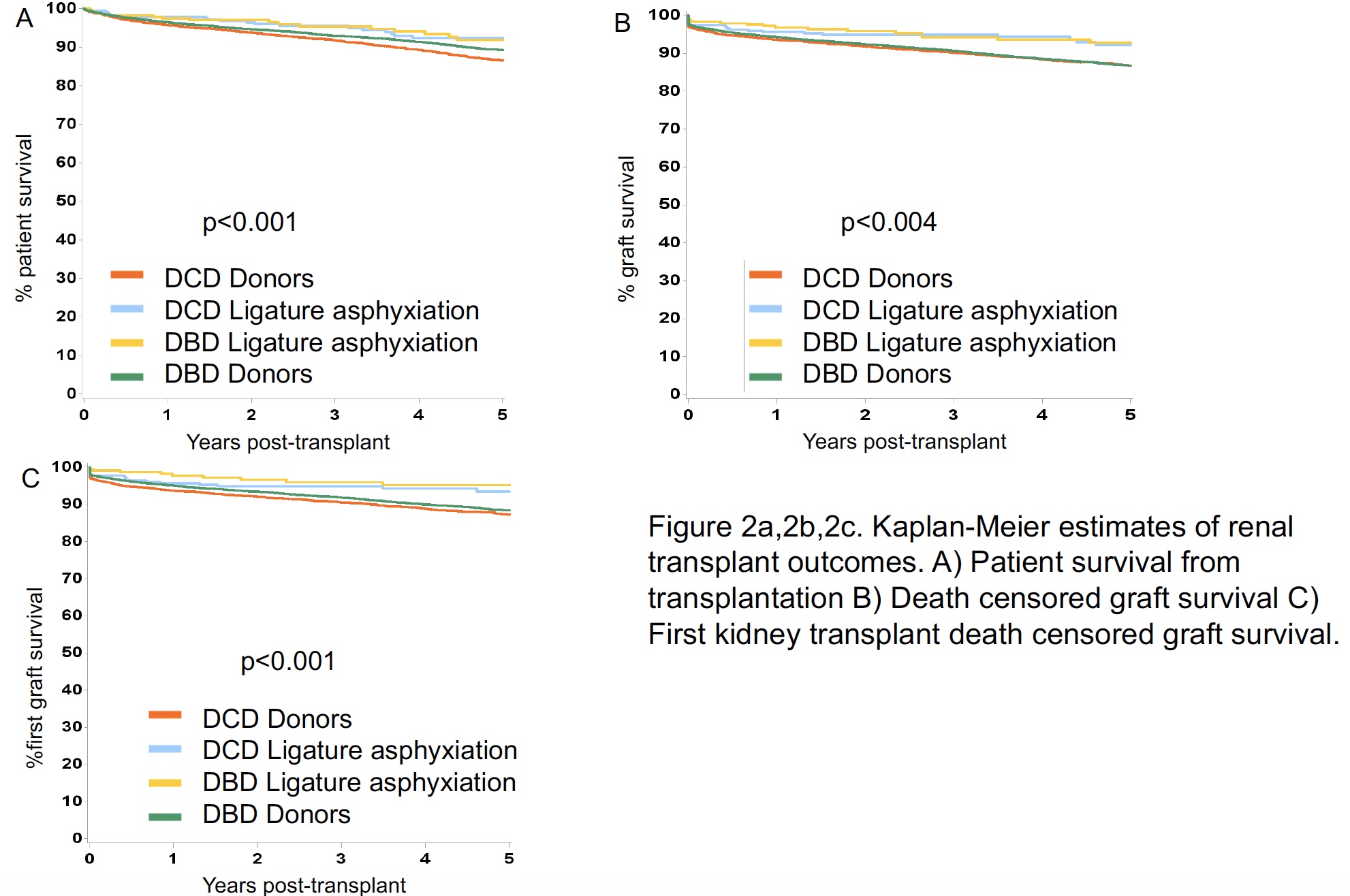 After adjusting for the differences in donor and recipient characteristics, donor ligature asphyxiation was not an independent predictor of 1 and 5 year patient survival or 1 year death censored graft survival. However, it was an independent predictor of good 5 year death censored graft survival (HR 0.712 (0.513-0.990), p=0.042)).
After adjusting for the differences in donor and recipient characteristics, donor ligature asphyxiation was not an independent predictor of 1 and 5 year patient survival or 1 year death censored graft survival. However, it was an independent predictor of good 5 year death censored graft survival (HR 0.712 (0.513-0.990), p=0.042)).
Discussion: Organ donors who die following ligature asphyxiation represent a relatively small but important proportion of the overall deceased donor population. The findings from the present analysis show that use of kidneys from both DBD and DCD donors who died following ligature asphyxiation result in excellent transplant outcomes.
Conclusions: In view of the above, increased consideration should be given to the use of kidneys from potential donors following ligature asphyxiation.
The National Institute of Health Research, Blood and Transplant Research Unit (NIHR BTRU) on Organ Donation and Transplantation at the University of Cambridge in collaboration with Newcastle University and in partnership funded this research with NHS Blood and Transplant (NHSBT). .

