
Intraoperative Retrograde Intrarenal Surgery (RIRS) as a Good Management Option for Large Ureteropelvic Impacted Stone of Transplanted Kidney
Giuseppe Ietto1, Gabriele Soldini1, Domenico Iovino1, Cristiano Parise1, Elia Zani1, Veronica Raveglia1, Giovanni Saredi1, Matteo Tozzi1, Giulio Carcano1, Francesco Amico1.
1General and Trasplant Surgery, University of Insubria, Varese, Italy
Introduction: Urolithiasis is a rare complication following kidney transplantation. Many of the clinical features of urinary stones after transplantation differ from those of non- transplant patients, but the course is essentially similar to that in non-transplant patients with lithiasis. The management of kidney stones has evolved radically over the years and involved extracorporeal shock wave lithotripsy (ESWL), flexible ureteroscopy and in situ lithotripsy, percutaneous nephrolithotomy (PCNL), open pyelolithotomy and open cystolitholapaxy. Retrograde URS with laser lithotripsy and/or basket extraction is a reasonable option for treating small and large stones also in transplanted kidney. In order to overcome the difficulty of complex anatomy typical of non-native ureter, ureteroscope can be introduced through a small surgical ureterotomy allowing quite complete stones clear.
Matherials and Methods: We present surgical treatment and outcome in a 69-year-old male patient with a large ureteropelvic impacted stone of transplanted kidney one year and three months after transplantation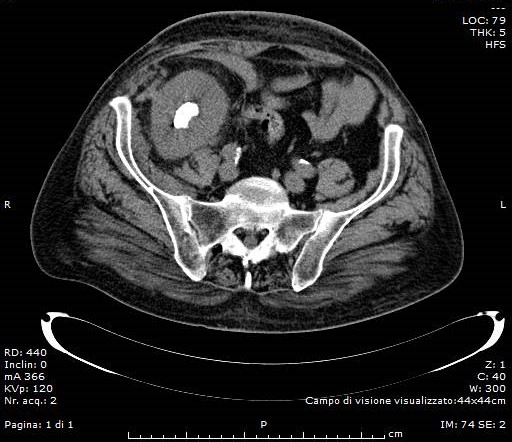
The transplated ureter and the ureteroneocystotomy was identified at the right anterior bladder wall. Ureterotomy was performend on the third part of transplated urether, the double J stent was removed and the ureter was eventually cannulated. Retrograde pyelography revealed an angulation of the mid-ureter toward the renal pelvis seen medially. Access was established with both a standard teflon wire and a superstiff teflon guidewire. A flexible ureteroscope was advanced beyond the midureter through ureterotomy into the transplanted kidney. Laser lithotripsy was then effectively performed in the standard manner by means of 200/273μm Holmium laser fibers. A tipless nitinol basket was used to extract the fragments.
Discussion: Native anatomy makes ureteroscopy simple. The orthotopic location of the ureteral orifices allow the urologist to take advantage of the bladder trigone as a backbone to advance wires and ureteroscopes. This is lost in cases as in that one described previously, where the non-native ureter is in a more anterior location.
The last attempt to remove pelvic stones in trasplanted kidneys is to introduce the ureteroscope through surgical ureterotomy. In this way is possible to avoid surgical incision of renal pelvis itself which is very difficult to isolate considering its proximity to vascular structures.
Conclusion: Upper urinary tract endoscopy has long been established as a safe and efficient means of managing urolithiasis with great success. With technological advances, ureteroscopy has evolved into a powerful tool in the armamentarium of the urologist. Management of patients with complex anatomy is now possible while avoiding more invasive interventions such as percutaneous nephrostolithotomy or surgical pyelotomie.

