
Perfusion parameters during Hypothermic Machine Perfusion in Expanded Criteria Donors (ECD) and Donors after Circulatory Death (DCD). Does comparison allow their categorization?
Victoria Gomez dos Santos1, Mercedes Ruiz1, Victor Diez Nicolás1, Sara Alvarez1, Vital Hevia1, Sandra Elias2, Francisco Javier Burgos1.
1Urology, Hospital Ramón y Cajal. Alcalá University, Madrid, Spain; 2Nephrology, Hospital Ramón y Cajal, Madrid, Spain
Urology Surgery and Transplantation Group. IRYCIS.
Introduction: ECD represent up to 80% of kidney transplant (KT) activity at our Center, which has also received and accepted DCD imported grafts.
HMP decreases the incidence of PNF and DGF, and increases 1-year graft survival compared to standard simple cold storage in ECD, moreover HMP decreases DGF in DCD. Flow and Renal Resistance (RR) during perfusion are used as graft viability parameters.
The aim of the study was to compare donor and recipient characteristics as well as perfusion Materials and Methods: Study data were prospectively collected in a cohort of consecutive first KT recipients from ECD and imported type II and III DCD between February 2012 and September 2017 with a minimum 6 months follow-up. Local kidneys were placed on Life-Port in the donor operating room and delivered to the recipient on the pump. Kidneys imported from other organ procurement hospitals were initially placed on ice until reaching our center.
Early graft loss, DGF, kidney function at 1 year post-KT and acute rejection were considered.
Quantitative data were expressed as mean (SD) or median (IQA) and qualitative data as ratios. Comparison was conducted using Student t test; Mann-Whitney, Fischer or Chi squared as appropriate. Statistical significance was established at p<0.05.
Results: 230 recipients from ECD and 20 from DCD were included. DCD donors were significantly younger as expected (72.8 years vs 59.0 p= 0.00). There were no differences in respect to sex, final creatinine and main comorbidities except hypertension. Cold ischemia time was longer in ECD (17.5 hours vs 15.2; p= 0.045) although relative machine perfusion time were similar. Recipients from ECD were older and more frequently male but there were no differences in comorbidities and time in dialysis.
Machine perfusion parameters didn´t show any difference at any time point, nevertheless flow and RI evolution through perfusion was as expected, with a significant increase in flow and corresponding decrease in RI (Table 1).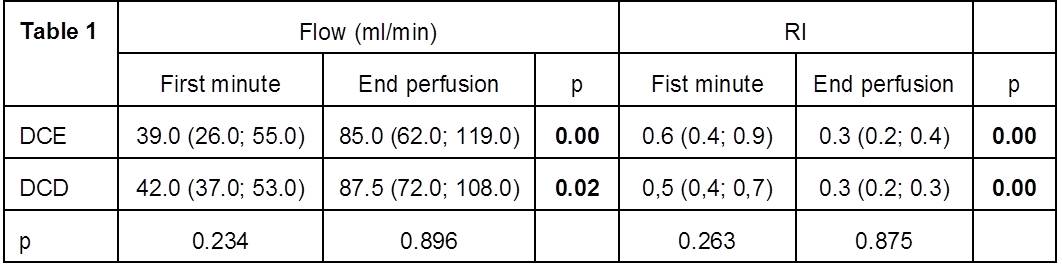
Finally, DCD showed significantly more frequent DGF (47.4% vs 18.0%; p=0.001) and worse graft survival at 1 year (65.0% vs 83.3%; p=0,043). There were no differences in kidney function at 1 year in those functioning grafts (36.1 ml/min vs 40.7) (Table 2).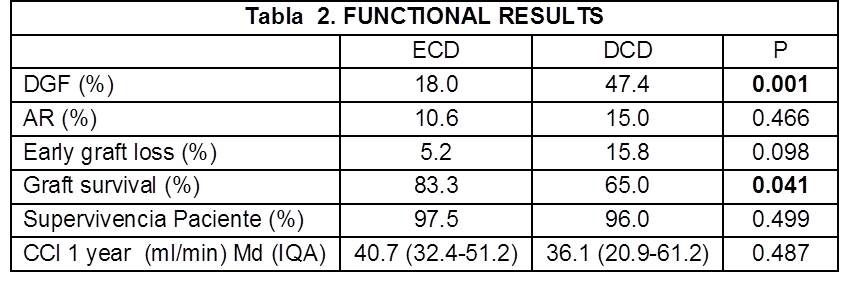
Conclusion: DCD functional results were inferior to those obtained in ECD despite its HMP. Perfusion parameters (flow and resistance) had the usual behavior in both groups and didn`t allow to categorize their source. In the actual state of knowledge, results improvement in DCD KT involves an effort in decreasing and tight controlling cold ischemia time.

