
Modified DFPP Eliminates ABO Blood Type IgG Antibody with Preserving Fibrinogen before ABO-Incompatible Kidney Transplantation
Daiki Iwami1, Takenao Matsumoto2, Kiyohiko Hotta1, Minoru Ota2, Yuki Chiba2, Haruka Higuchi1, Nobuo Shinohara1.
1Department of Urology, Hokkaido University Hospital, Sapporo, Japan; 2Medical Engineering Center, Hokkaido University Hospital, Sapporo, Japan
Introduction: Safe and effective elimination of ABO blood type antibody is critical before ABO-incompatible kidney transplantation (ABOi KTx). Plasma exchange (PEx) has the risks of hyperacute allergic reactions and microorganism transmission caused by using fresh frozen plasma. Another apheresis Double filtration plasmapheresis (DFPP) using albumin solution removes antibodies effectively, however, fibrinogen (Fib) is massively removed resulting in hemostasis failure. Unfortunately, immunoadsorption hasn’t been approved by health insurance in Japan, yet. Therefore, we created a modified combination of filtrating membranes in DFPP (modified DFPP, mDFPP) to retain more Fib while removing IgG, and assessed its efficacy and safety in comparison with conventional DFPP (cDFPP).
Materials and Methods: Patients who underwent ABOi KTx were enrolled in the study. As a primary plasma separator, we used Plasmaflo® OP-08W in cDFPP and Cascadeflo® EC-50W, whose pore size is smaller than OP-08W to filtrate large molecules including Fib back to patient’s plasma, in mDFPP, respectively. Cascadeflo® EC-20W was used as a secondary separator in both DFPP. Removal rates (RR) of IgG antibodies and Fib after each DFPP per session were compared between cDFPP and mDFPP. Incidence of adverse events during and after each DFPP was compared between the groups.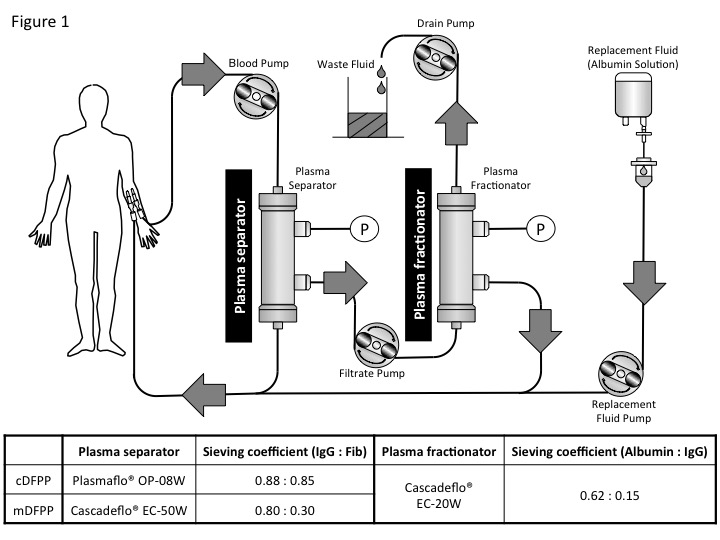
Results: cDFPP and mDFPP were performed in 16 and 10 cases, respectively. The patient’s clinical backgrounds were similar between the groups. RR of IgG and IgM were both significantly lower in mDFPP than in cDFPP (IgG, 62.1±6.7% vs 74.6±9.6%, p<0.001, and IgM, 84.2±8.8% vs 15.0±5.2%, p<0.001). Similarly, ABO IgG titers drop was significantly lower in mDFPP than in cDFPP (2.0±0.7 vs 1.2±0.4, p=0.039). However, loss rate of Fib was significantly lower in mDFPP than in cDFPP (38.1±11.5% vs 75.5±5.3%, p<0.001). Regarding adverse events, there was no hypotension event observed in either DFPP treatment, however, incidence of hemostasis prolongation of arteriovenous fistula was significantly higher in cDFPP group (81.8%) than in mDFPP group (12.5%), suggesting that mDFPP preserve more Fib than cDFPP, resulting in better hemostasis.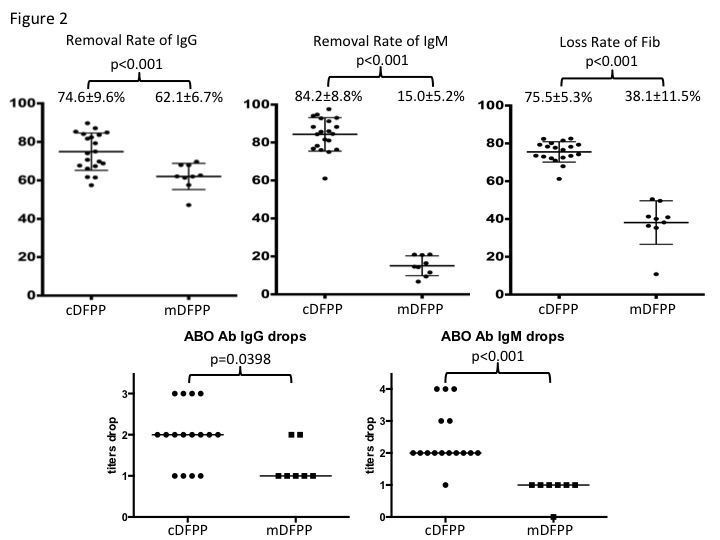
Discussion: Our results suggested that mDFPP removes both IgG and IgM antibodies significantly less than cDFPP, however, the actual difference in RR of IgG seems acceptable and mDFPP can preserve much more coagulant factors such as Fib. Collectively, mDFPP can be advantageous in performing during perioperative period to remove selectively IgG ABO antibody for ABOi KTx.
Conclusions: mDFPP is effective and safe apheresis to remove ABO blood type IgG antibody selectively before ABOi KTx.
Kota Ono. Sachiyo Murai.

