
Head to Head Comparison of Speckle Tracking Strain Echocardiography with Invasive Hemodynamic Assessment for the Detection of Acute Cellular Rejection in Cardiac Allograft Recipients
Leyla Elif Sade1, Serpil Eroglu1, Bahar Pirat1, Atilla Sezgin2, Alp Aydinalp1, Handan Ozdemir3, Haldun Muderrisoglu1.
1Cardiology, Baskent University, Ankara, Turkey; 2Cardiovascular Surgery, Baskent University, Ankara, Turkey; 3Pathology, Baskent University, Ankara, Turkey
Introduction: Non-invasive alternatives to endomyocardial biopsy (EMB) are highly desirable to monitor acute cellular rejection (ACR). In the present study, we aimed to test the hypothesis that echocardiographic strain quantification, by tracking subtle alterations in myocardial function, is useful and superior to invasive hemodynamic measurements to detect ACR.
Materials and Methods: All patients underwent serial surveillance EMBs, catheterizations and echocardiography examination according to our institutional protocol. Data from the first rejection episodes were compared with the data obtained after treatment. Patients without rejection during follow-up were also included for comparison. All tests were performed within 48 hours of each other. In addition to standard 2D and Doppler echocardiographic measurements, global longitudinal and circumferential strain (GLS, GCS) were assessed from 16 segments, from digitally stored echocardiograms by using the Velocity Vector Imaging software on Syngo Workplace (Siemens Healthcare GmbH, Erlangen/Germany).
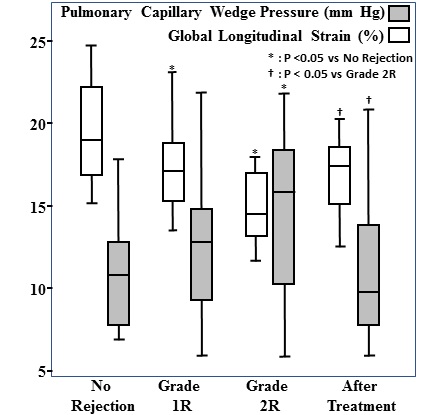
Results: We observed 16 grade 1R, 14 grade 2R and 1 grade 3R and 18 no rejection. Time to first rejection was 3 months (interquartile range: 3-36). Only GLS and GCS were significantly reduced during grade 1R. During grade ≥2R, GLS, GCS, tricuspid annular peak systolic excursion, cardiac index were significantly reduced, right atrial and systolic pulmonary artery pressures were significantly increased as compared to no rejection. The negative and positive predictive values of the best fit cut-off of GLS (<17%) were 98% and 43% for grade ≥2R, 84% and 70% for any rejection. In the multivariate logistic regression analysis including the most pertinent variables according to univariate analyses, GLS and GCS emerged as independent determinants of any rejection (p=.015 and p=.004, respectively). Despite successful treatment, strain values remained significantly lower than the values of no-rejection group (GLS 17.0% [14.7% - 18.3%] vs 18.9% [16.8% - 22.1%]; p=.006, GCS 25.5% [22% - 27.8%] vs 29.0% [24.0% - 33.4%]; p=.01).
Conclusions: Echocardiographic strain, but not hemodynamic assessment by cardiac catheterization, is a sensitive tool to detect first rejection episode after HTx. However, incomplete normalization of strain after treatment necessitate intra-individual comparisons on serial follow-up are warranted. Strain is a promising marker of ACR however it needs to be tested in larger series.

