

Concentric Left Ventricular Hypertrophy Geometry Predicts Cardiovascular Events After Renal Transplantation
Edoardo EM Melilli Phd1, Laura MV Martinez Valenzuela MD1, Sergi SC Codina MD1, Ariel AT Tango MD1, Anna AM Manonelles MD1, Nuria NM Montero Perez MD 11, Eduard EC Claver MD2, Oriol OB Bestard Phd1, JosepMaria JMC Cruzado Phd1.
1Renal Transplant Unit, Bellvitge Hospital , Barcelona, Spain; 2Cardiology Imaging Unit, Bellvitge Hospital, Barcelona, Spain
Background and Objectives: Chronic kidney disease population, even after kidney transplant, is at higher risk of cardiovascular events. The aim of the study is to evaluate the relationship between pre-transplant echocardiographic assessment of left ventricular abnormalities and post-transplant cardiovascular events occurrence.
Study Design and Setting, Participants and Measurements: Retrospective cohorts observational study, including 231 consecutive kidney transplant patients from Bellvitge University Hospital between 2010 and 2013 accounting with echocardiographic evaluation up to one year before kidney transplant. Patients were classified depending on its left ventricle morphology and mass into four categories (concentric hypertrophy, eccentric hypertrophy, concentric remodeling and normal geometry). Left ventricle mass was indexed to body surface area. Clinical and analytical data was also gathered. The primary outcome was a composite of cardiovascular events (congestive heart failure, acute coronary syndrome, cardiac sudden death, ictus and aortic aneurism rupture). Renal outcomes, and cardiac and overall mortality was also recorded.
Results: Using the classical definition of LVH, our study found a prevalence of 71 % for LVH in patients screened for waiting list inclusion, similar to previously described prevalence of LVH in dialysis patients. The mean LVMI in our patients was higher compared to general population, indicating the need for other echocardiographic findings to define cardiovascular risk.
Of note mean LVMI was 130,43 ± 42,27 g/m2. 164 (71,6%) patients accomplished the previously described left ventricular hypertrophy criteria. 44 patients (18.2 %) were classified as normal geometry, 22 patients (9.6 %) patients as concentric remodeling, 86 patients (37.6 %) as concentric hypertrophy, and 79 patients (34.6 %) as eccentric hypertrophy. LVMI was higher in concentric group compared to all others groups (p. < 0.001 compared to each other group). Figure 1 shows mean left ventricular mass index among geometry groups. 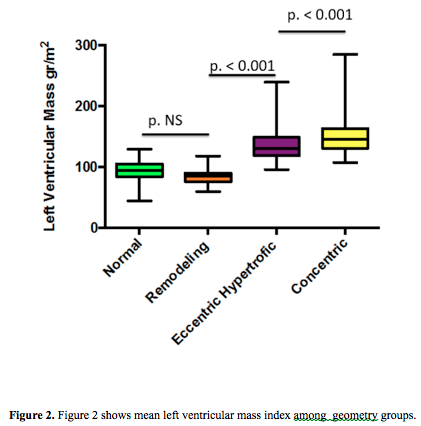
Table 1 shows basal population characteristics according geometric pattern.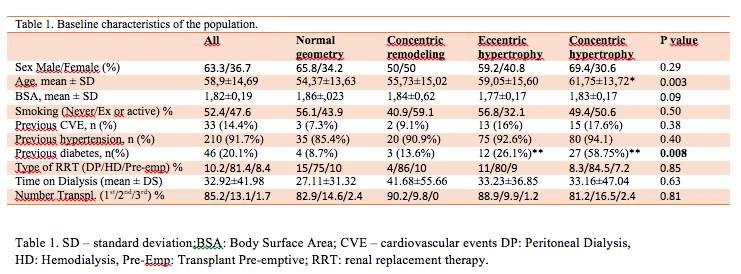
At kaplan mayer analysis, patients with concentric pattern had lower cardiovascular free events survival compared with others group (Log Rank 0.002 - see Figure 2 ) 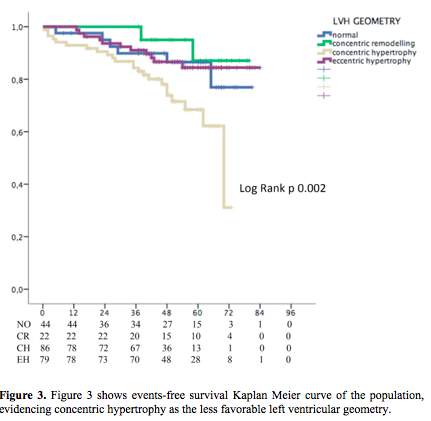
At cox regression logistic analysis concentric hypertrophy increases the risk of cardiovascular events comparing to the rest of geometric patterns (HR 2.753 CI 1.368-5.542 p=0.005). Every g/m2 increase on left ventricular mass (compared to the mean of our population) represents a 1.08 fold risk for cardiovascular events (HR 1.08 1.002-1.014 p value 0.005).
Conclusions: left ventricular geometry is a simple and useful parameter to stratify patients after kidney transplant by risk of cardiovascular events as earlier as from pre-transplant evaluation.

