Is Banff 2013 Classification of Renal Allograft Pathology Superior to 2007 Banff in Detecting and Managing Cases of Antibody-Mediated Rejection?
Jose Torrealba1, Daniel Burguete2, Jared Hassler1, Venkatesh Kuma Kumar1, Bekir Tanriover1, Allen Hendricks1.
1Pathology, University of Texas Southwestern Medical Center, Dallas, TX, United States; 2School of Medicine, University of Texas Southwestern Medical Center, Dallas, TX, United States
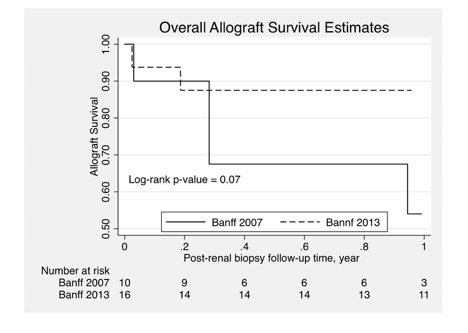
The 2013 Banff meeting updated the requirements for the diagnosis of acute/active antibody-mediated rejection (AAMR) in kidney allografts. There has been speculation that the changes lower the threshold for diagnosing AAMR, and may lead to possible unnecessary and expensive treatment. We compared the 2013 Banff classification for AAMR to the previous 2007 Banff to determine if there was an increase in the number of patients receiving a diagnosis of AAMR and if the diagnosis affected allograft survival and post-biopsy 3-month and 6-month creatinine and eGFR values. We reviewed all renal allograft biopsies occurring at a single institution from Aug. 2012 to Aug. 2016. 134 patients (212 renal allograft biopsies) were identified and were compared to both 2007 and 2013 Banff classification requirements for AAMR. 10 patients (11 biopsies) met 2007 criteria. An additional 15 patients (20 biopsies) met 2013 criteria. These two groups showed no statistically significant demographic differences. By applying the 2013 Banff classification, we observed a 2.5 fold increase in the number of AAMR cases. One-year post-transplant allograft survival was higher in the 2013 group (0.85 vs. 0.55) but was not statistically significant (p <0.07), Fig. 1. The 3-month and 6-month post-biopsy creatinine values were significantly lower for the 2013 group (1.6 ± 0.6 vs. 3.3 ± 2.2, p value 0.01 and 1.7 ± 0.6 vs. 3.4 ± 2.8, p value 0.03). The 3-month and 6-month eGFR values were higher in the 2013 group, although not statistically significant. These results show the 2013 Banff classification to be superior to Banff 2007 for detecting milder and earlier cases of AAMR leading to earlier initiation of treatment and subsequent increased allograft survival and improved 3-month and 6-month creatinine and eGFR values.