
Correlation between CT Volumetry and Nuclear Medicine Split Renal Function in Live Kidney Donation - A Single Centre Experience
Lina Hua1,2, Ruben Sebben3, Santosh Olakkengil1, Christine Russell1, Shantanu Bhattacharjya1.
1Department of Surgery, Central Adelaide Local Health Network , Adelaide, Australia; 2Department of Surgery, Northern Adelaide Local Health Network, Adelaide, Australia; 3Department of Medical Imaging, Central Adelaide Local Health Network, Adelaide, Australia
Introduction: Potential live renal donors undergo renal computed tomography angiogram (CTA) and nuclear imaging dimercaptusuccinc acid (DMSA) scans as part of their work up. CTA provides information about the anatomical structure of the kidney, whilst DMSA is considered the scan of choice for evaluating differential renal function and potential scarring. However, DMSA results are influenced by donor body habitus, kidney location, examiner, and operator disparity. The need for both imaging modalities adds another investigation for the patient, potential delays in treatment, and additional costs to the healthcare system.
Aim: The aim of this study was to determine the relationship between split renal volumes measured on CTA and renal volumes derived from DMSA in live renal donors.
Methodology: Prospectively collected data of 58 consecutive patients who underwent live laparoscopic donor nephrectomy at a single centre from 2014-2017 was reviewed. Only patients who had preoperative CTA and DMSA imaging were included. 3D reconstruction of the kidney was generated from the arterial phase CTA images using Carestream software. One investigator confirmed the renal tissue of interest prior to automated software calculation of renal volume on CTA. Split function renal volume was compared against calculated DMSA split volume (percentage split function multiplied by total renal volume).
Results: There were 58 live donor nephrectomies in this period. 5 were excluded because of incomplete data. 53 patients were studied. Pearson coefficient was 0.95 for right renal volume, and 0.95 on left renal volume measured on CTA and calculated on DMSA. 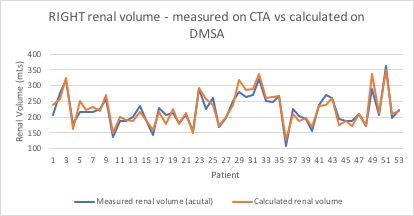
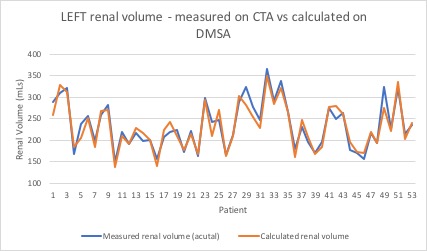
Discussion: In our cohort, split renal volumes measured on 3D images obtained from CTA correlate to calculated split volumes based on renal function determined from DMSA.
In keeping with the aims of live donation in leaving the donor with the kidney with better function our results would suggest that this decision can equally be arrived at with CT renal volumetry alone.
Dropping a DMSA scan in the evaluation of a kidney donor reduces the radiation load by 0.70mSv equivalent to 35 chest x rays; and a cost saving of $430.00 per donor.
Conclusion: Current CT technology allows accurate assessment of renal volumes that correlate well with DMSA split function.
The decision of which kidney to donate is based on function and anatomy which can be achieved with A CTA as a one stop shop.
Avoiding a DMSA scan results cost reduction as well as radiation in the assessment of a live donor.

