
The Role of Proteinuria, Paricalcitol and Vitamin D in the Development of Post-Transplant Diabetes Mellitus after Kidney Transplantation
Ivana Dedinska1, Juraj Miklušica1, Ľudovít Laca1, Petra Skalová1, Peter Galajda2, Marián Mokáň2.
1Surgical Clinic and Transplant Center, University Hospital Martin and Jessenius Faculty of Medicine Comenius University, Martin, Slovakia (Slovak Republic); 2Internal Clinic I, University Hospital Martin and Jessenius Faculty of Medicine Comenius University, Martin, Slovakia (Slovak Republic)
Introduction: The post-transplant diabetes mellitus (PTDM) occurs most frequently during the first year after the transplantation. We focused on parameters of calcium-phosphate metabolism and proteinuria as possible new risk factors for PTDM after kidney transplantation.
Materials and Methods: We have prospectively identified in a set of 167 patients after kidney transplantation risk factors for post-transplant diabetes mellitus with follow-up of 12 months. Patients with diabetes mellitus type 1 and type 2 as well as patients using ciclosporin A or mTOR inhibitor have been excluded from the monitoring. From the perspective of immunosuppression it was a homogeneous set of patients.
Results: We identified the following independent risk factors for PTDM in our set: average proteinuria >0,300 g/24 hours [HR 3.0785, (95 % CI 1.6946-5.5927), P = 0.0002], level of vitamin D < 20 ng/ml [HR 5.4517, (95 % CI 2.3167-11.8209), P <0.0001] base line serum level of phosphorus >1.45 mmol/l [HR0.0821, (95 % CI0.0042-1.5920), P = 0.0439]. 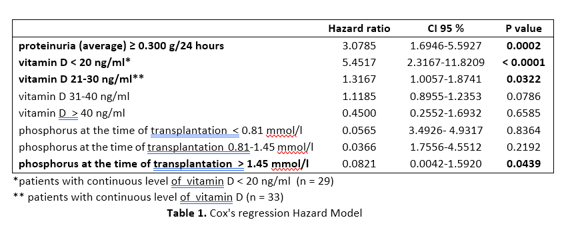 The lowest occurrence of PTDM and proteinuria was recorded in patients whose treatment included paricalcitol (P <0.0001) and these patients had at the same time the highest level of vitamin D (P <0.0001).
The lowest occurrence of PTDM and proteinuria was recorded in patients whose treatment included paricalcitol (P <0.0001) and these patients had at the same time the highest level of vitamin D (P <0.0001).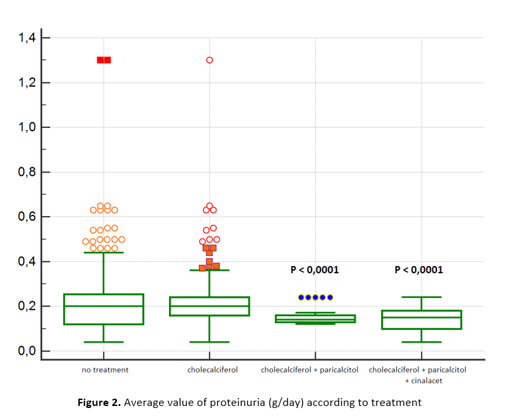
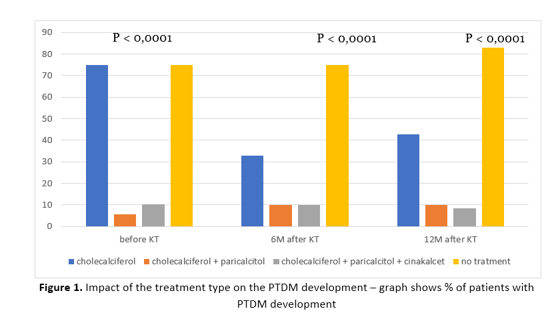
Conclusion: Deficit of vitamin D, proteinuria and hyperphosphatemia are independent risk factors for the development of PTDM in our set. We identified the usage of paricalcitol as protective factor with regard to the PTDM development.

