
Anesthesiologic Management for Multivisceral Transplant: A Case Report
Meta Levstek1, Adriana Calderon Barajas1, Aida Fernandez García1, Adolfo García Gutierrez1, Angel Callejo Martín1, Claudia Olea Vielba1, Manuel Cortes Guerrero1, Francisco Perez-Cerdá Silvestre1.
1Anesthesiology and Critical Care, University Hospital Doce de Octubre, Madrid, Spain
Introduction: Multivisceral transplantation (MVTx) is en block transplantation of three or more abdominal organs for patients with irreversible abdominal organ failure or unresectable gastrointestinal or mesenteric masses. It is an uncommon procedure but represents a challenge for anesthesiologist for its complexity and important hemodynamic and metabolic instability.

Matherials and Methods: 42y old female, with history of bariatric surgery (sleeve gastrectomy), total colectomy for familial adenomatous polyposis and one pregnancy, undergoes MVTx due to unresectable desmoid tumor of small bowel and data of hyperimmunization. Standard monitorization and rapid sequence induction of general anesthesia is carried out. Pulmonary artery catheter is placed for hemodynamic monitoring and blood products therapy is done using ROTEM®. During the extenteration (phase I) the patient needs norepinephrine and presents steady rise of lactic acid with metabolic acidosis that is corrected. A perfusion of rapid acting insulin is initiated at the end of this phase. Blood volume is optimized before the reperfusion with 1,5L of blood products to treat massive fluid shift. During the reperfusion we administer epinephrine, calcium chloride and sodium bicarbonate and continue with norepinephrine. There is no postreperfusion syndrome. The lactic acid peaks 3h after reperfusion. A perfusion of tranexamic acid is added due to diffuse bleeding. The patient is transferred intubated to an intensive care unit.
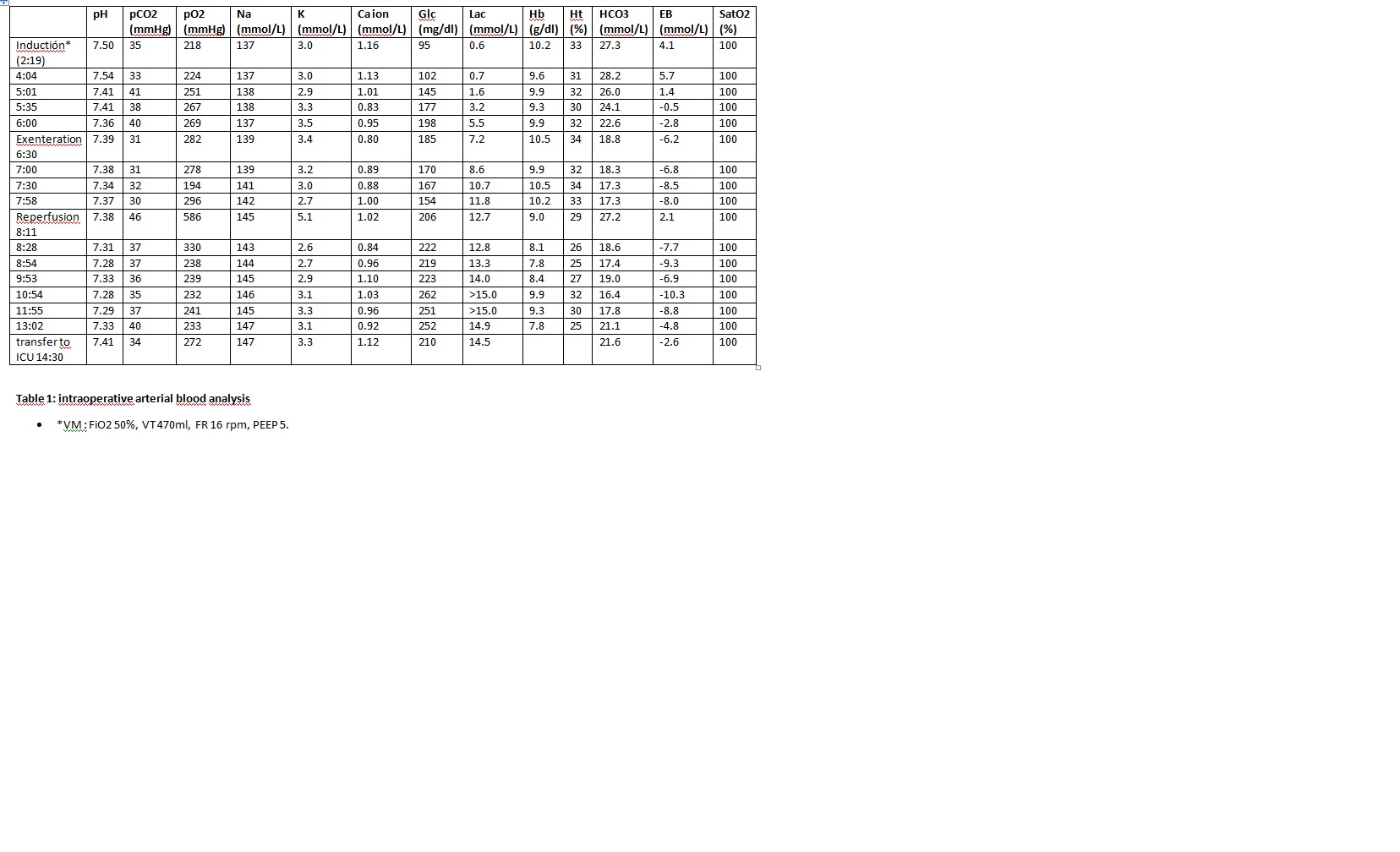
Results and Discussion: Our patient was relatively stable with norepinephrine perfusion (up to 0.3mcg/mg/min). The curve of lactic acid followed a course showed in other studies. During the phase I our goal was to maintain hematocrit around 30-35% to avoid mayor hemodynamic changes during the reperfusion. She presented important coagulopathy throughout the whole surgery that was corrected with blood products and tranexamic acid guided by ROTEM®.
Due to the complexity of MVTx the candidates should undergo a detailed and multidisciplinary preoperative evaluation. For general anesthesia a rapid sequence induction should be performed because this patients present delayed gastric emptying. Venous access can be challenging due to venous thrombosis secondary to chronic parenteral nutrition. The monitorization should be extensive, preferably with continuous cardiac output and mixed-venous oxygen saturation and/or transesophageal echocardiography to asses preload and ventricular wall motion. A rapid infusion device is critical to overcome the massive volume shift at reperfusion and to help with maintenance of normothermia to avoid coagulopathy and cardiac instability.
Conclusion: The major critical points in MVTx are metabolic acidosis, hypotension, hyperlactacidemia, hyperkaliemia, hypocalcemia, hypothermia and coagulopathy associated to mayor bleeding. The role of anesthesiologist is to recognize this critical points and treat accordingly.

