
Pyloric Artery to Segment 4 Artery Vascular Reconstruction, a Novel Surgical Technique Developed for Donor Safety after LLS Hepatectomy, and now Proposed for Extended Right Lobe Split Grafts
Gabriel E Gondolesi1, Andres Fraile1, Luis M Mercado1, Diego A Ramisch1, Pablo Barros Schelotto1.
1Unidad de Hepatología, Cirugía HPB y Trasplante Hepático, Hospital Universitario Fundación Favaloro, Ciudad Autónoma de Buenos Aires, Argentina
Introduction: Strategies to increase the pull of organs include the use of segmental liver grafts. While performing left lateral segment (LLS) from a living donor, the transection of the left hepatic artery becomes critical when a dominant segment 4 artery (S4A) emerges higher from the main right and left bifurcation. Similar situation occurs while performing split procedures. In the living donor, it is mandatory to assure donor safety, while when using extended right lobe split grafts (ERLSG) an adequate arterial supply to segment 4 (S4) will reduce post-operative recipient morbidity.
Aim: We aim to describe a novel technique consisting on performing a pyloric to segment 4 arterial microsurgical reconstruction.
Report of cases: 1) A LLS 45 year old living donor was selected for a paediatric recipient, during the procedure a high dominant S4A was dissected, and in order to obtain an appropriate left HA length and diameter for the recipient, it was necessary to section it. Once the graft was removed from the field and in order to guarantee donor safety, the pyloric artery was dissected with a sufficient length to rotate it, and to perform a microsurgical anastomosis to the S4A.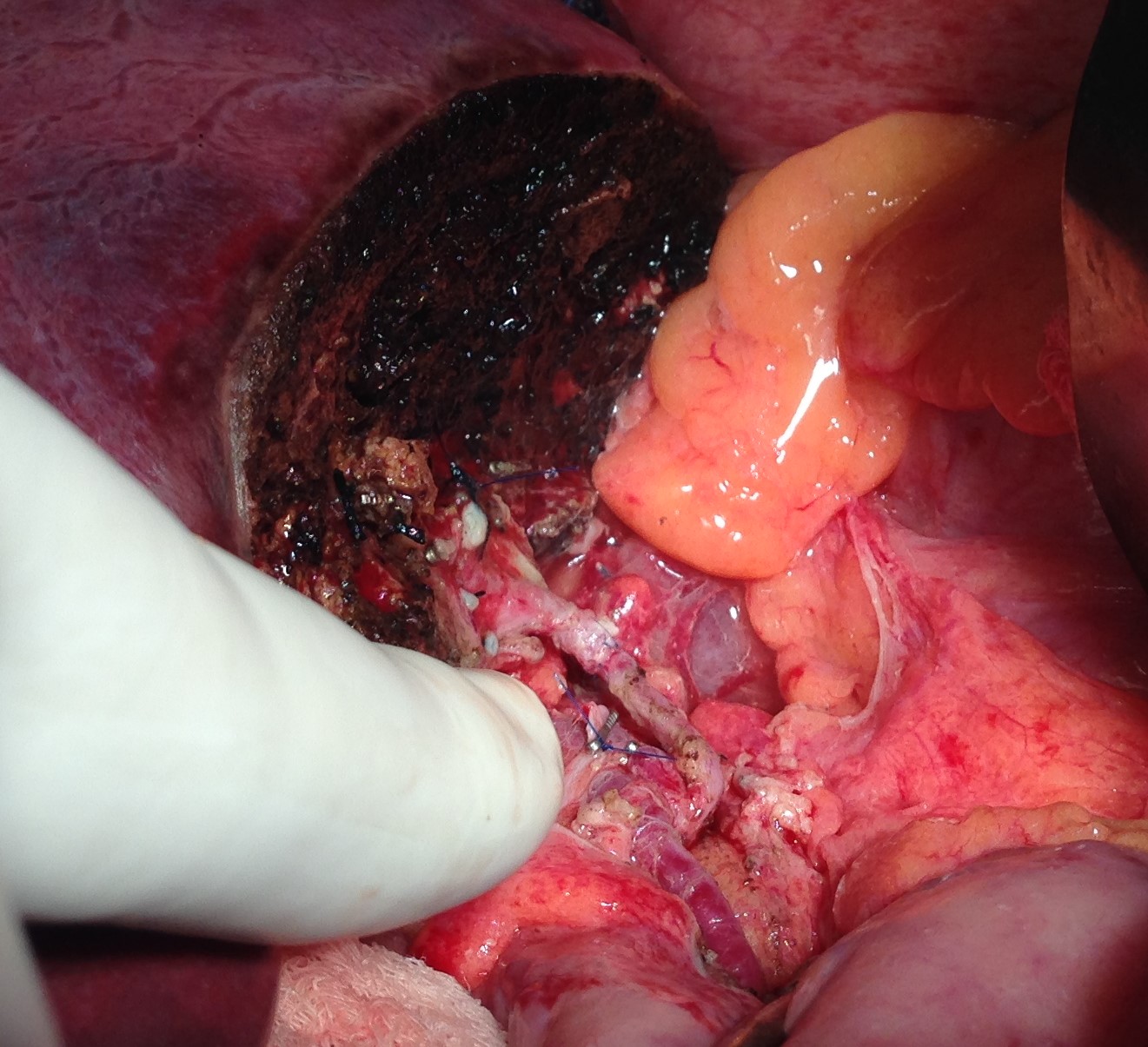 After reperfusion, the S4 recovered color and Doppler signal.
After reperfusion, the S4 recovered color and Doppler signal.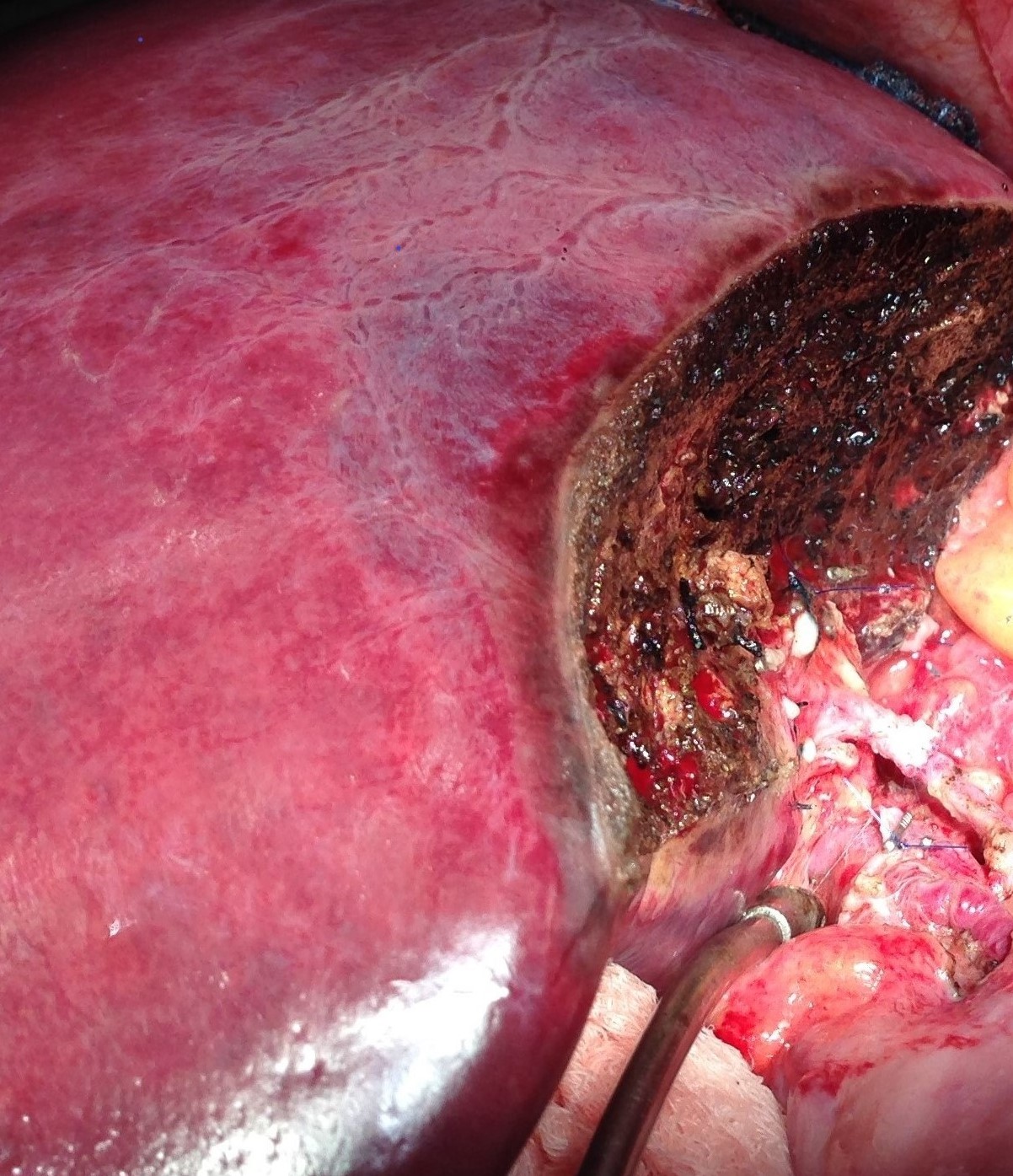 Reconstruction remains opened by CT scan angiogram 40 months after the procedure. 2) Similarly, during an ERLSG cadaveric LTx done in a 61 yrs old, HCV pt with HCC within Milan criteria, the S4A was found to be transected during the split procedure. After performing the portal and HAT reconstruction, the S4 remained incompletely perfused, therefore, the piloryc to S4A reconstruction allowed to recover color and Doppler signal.
Reconstruction remains opened by CT scan angiogram 40 months after the procedure. 2) Similarly, during an ERLSG cadaveric LTx done in a 61 yrs old, HCV pt with HCC within Milan criteria, the S4A was found to be transected during the split procedure. After performing the portal and HAT reconstruction, the S4 remained incompletely perfused, therefore, the piloryc to S4A reconstruction allowed to recover color and Doppler signal.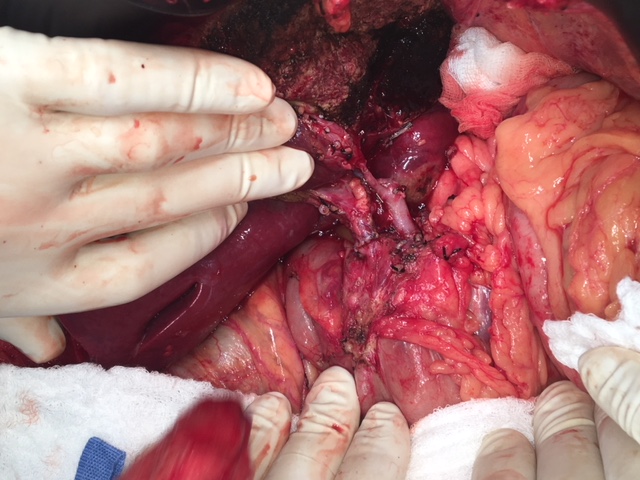 Reconstruction remains open by CT scan angiogram 3 months after the procedure.
Reconstruction remains open by CT scan angiogram 3 months after the procedure.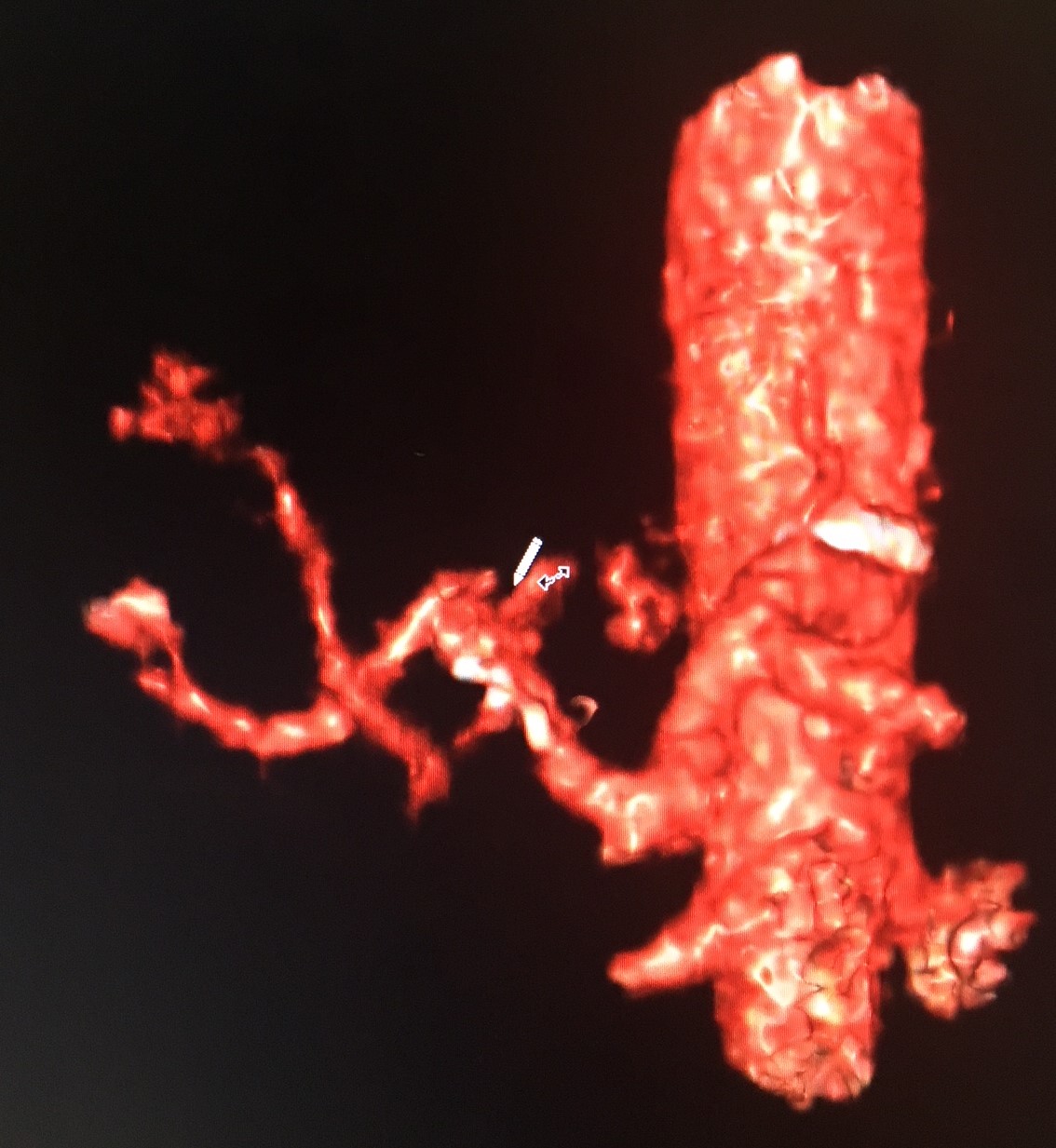 No biliary, or cut surface complications were seen in both cases
No biliary, or cut surface complications were seen in both cases
Conclusions: The described procedure it is a simple and novel technique that can be used for LLS and ERLSG. Its use might contribute to increase donor selection, and to reduce living donor and recipient S4 related complications.

