
IgA Nephropathy with Crescent Formation after Renal Transplantation
Raouya Grati1, Soumaya Chargui1, Mongi Bacha1, Raja Trabelsi 1, Khouloud Manai1, Hafedh Hedri1, Ezzedinee Abderrahim 1, Taieb Ben Abdallah1.
1Internal Medecine, Hospital Charles Nicolle , TUNIS, Tunisia
Background: Recurrent or de novo glomerulonephritis is an important cause of renal dysfunction after renal transplantation. Diagnosis is based on histological examination of renal biopsy .recurrent glomerulopathy is the massive frequent condition. IgA nephropathy (IgAN), the most common type of glomerulonephritis, histologically recurs in up to 60% of the patients. IgA nephropathy with crescent formation was rare. These patients showed rapidly progressive renal dysfunction and most of them lost graft function. It is no specific therapy other than optimal supportive care has been established and there is no recommendation to use immunosuppressive therapies to prevent the recurrence.
Case report: It is about a 42-year-old patient, in the antecedent of arterial hypertension, transplanted renal in 2012, from a kidney of related alive donor, because of a chronic renal disease of unknown etiology
The evolution after the transplant was marked by the arisen of a sarcoma of Kaposi in 2014, requiring putting him under rapamune after stop of any immunosuppressive treatment with a good evolution (complete forgiveness). He was hospitalized in September 2017 with a history of acute kidney injury and lower limbs edema. He presented a nephritic syndrome (albumin= 26.4/ protein=50), accompanied by an increase of urinary protein excretion (2 to 12 g/24H) without hematuria. The immunological balance was normal.
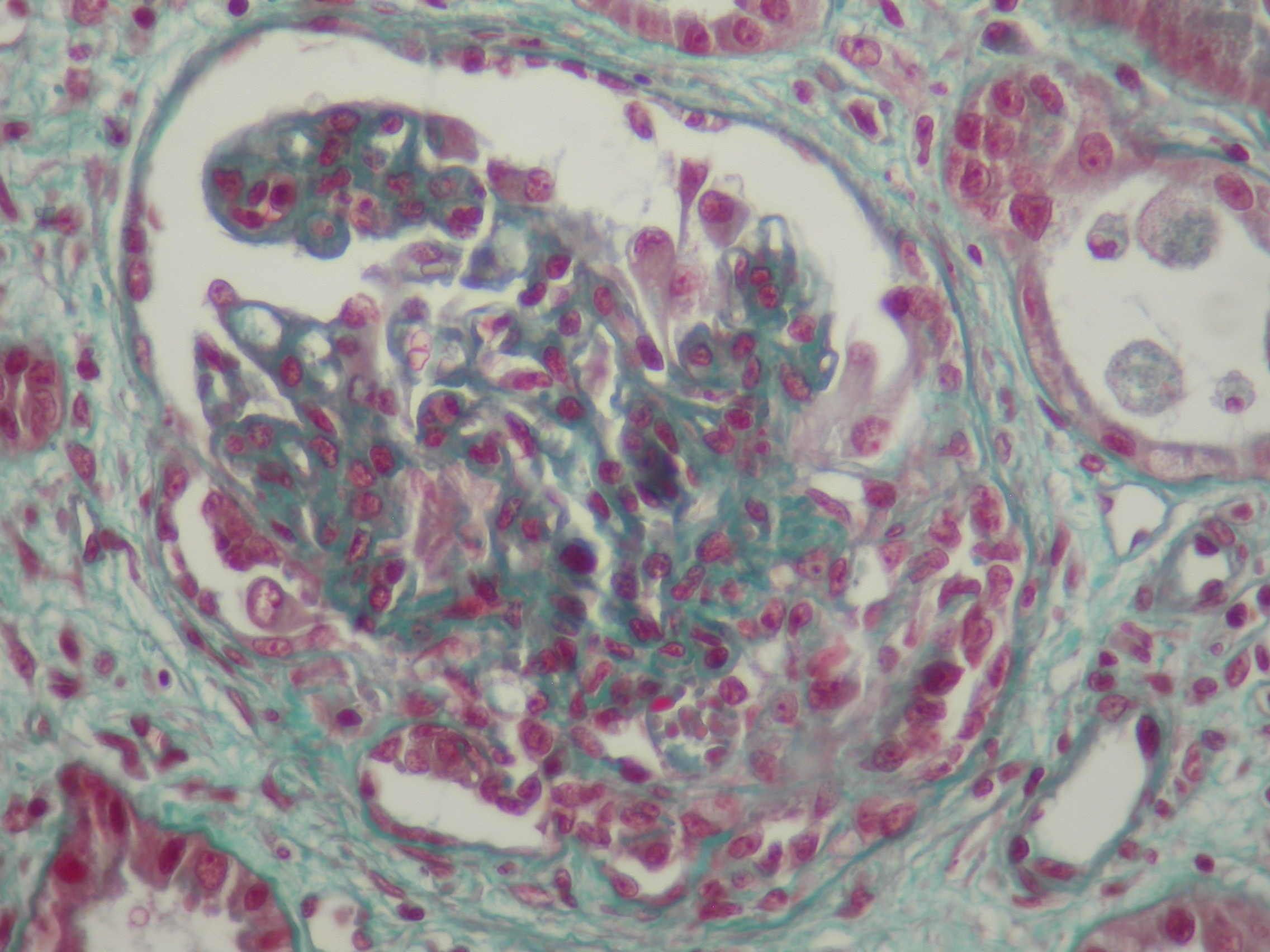
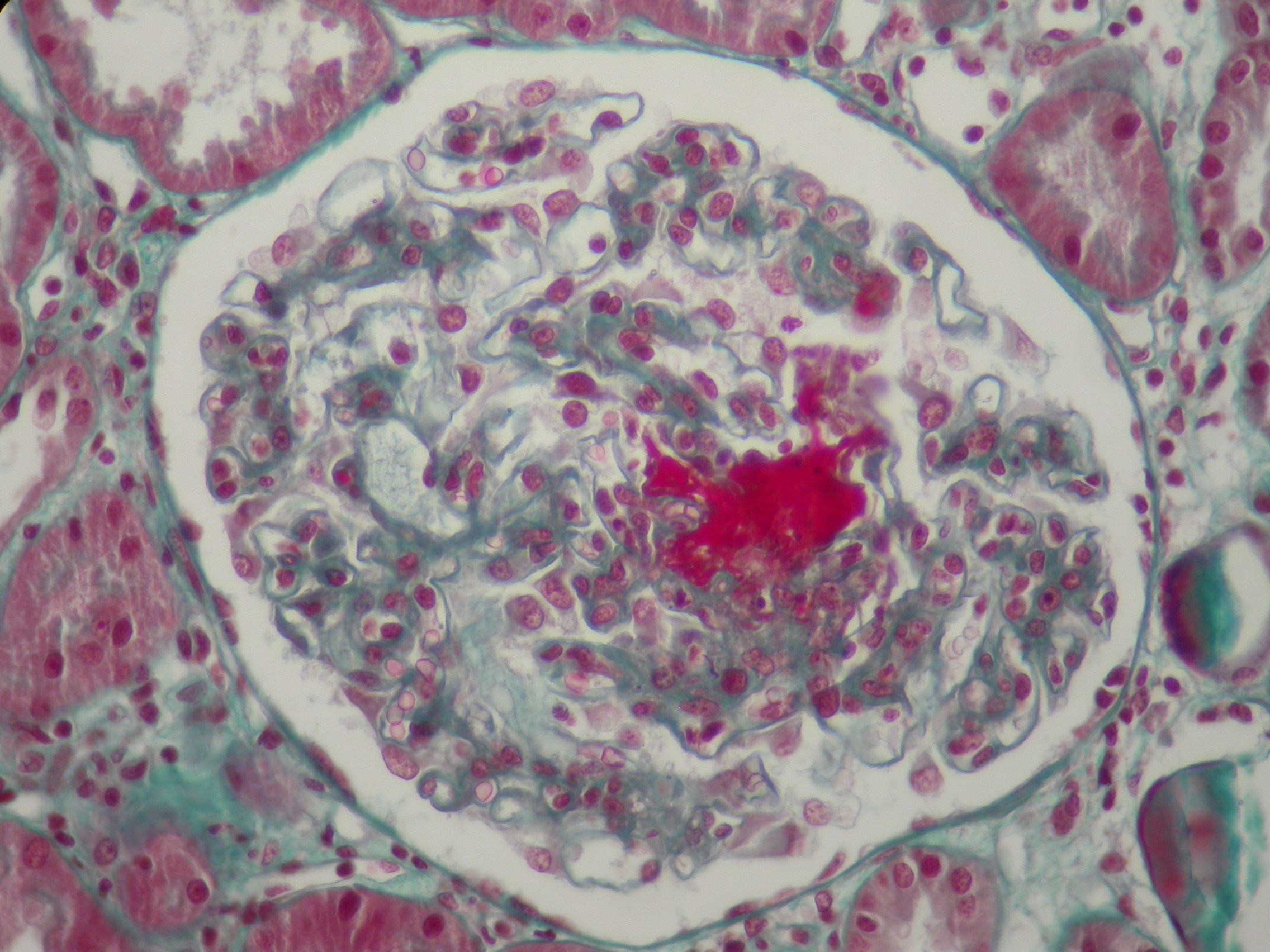
The renal biopsy showed mesangial proliferation, crescent formation and deposits of immunoglobulin A on immunofluorescence.
He received methyl prednisolone therapy (0.5 g intravenous injection per day for three times) relayed through oral corticosteroid such as prednisone 0.5 mg/kg every two days according to the protocol of POZZI.
After two months he kept stable renal function and decrease of urinary protein excretion (4g/24h).
Conclusion: In summary, IgA nephropathy with crescent formation was not always expressed by a rapidly progressive renal failure, such as the case of our patient.
There was never a consensus of treatment. We should forever prevent de novo or recurrence glomerulonephritis by a regular follow-up.

