Bortezomib Eliminates Plasma Cells from the Renal Graft in Plasma Cell-Rich Acute Rejection.
Masayuki Tasaki1, Kazuhide Saito1, Yuki Nakagawa1, Masahiro Ikeda1, Naofumi Imai2, Yumi Ito2, Takeshi Yamada3, Hiroya Hasegawa3, Kota Takahashi1, Yoshihiko Tomita1.
1Division of Urology, Department of Regenerative & Transplant Medicine, Graduate School of Medical and Dental Sciences, Niigata, Japan; 2Division of Clinical Nephrology and Rheumatology, Graduate School of Medical and Dental Sciences, Niigata, Japan; 3Department of Pediatrics, Graduate School of Medical and Dental Sciences, Niigata, Japan
Background: Plasma cell–rich acute rejection (PCAR) and antibody- mediated rejection (ABMR) are associated with poor graft survival, and a standard treatment has not yet been established. Bortezomib is a proteasome inhibitor that induces apoptosis of plasma cells; however, there have been no reports that bortezomib is effective for PCAR accompanied by ABMR.
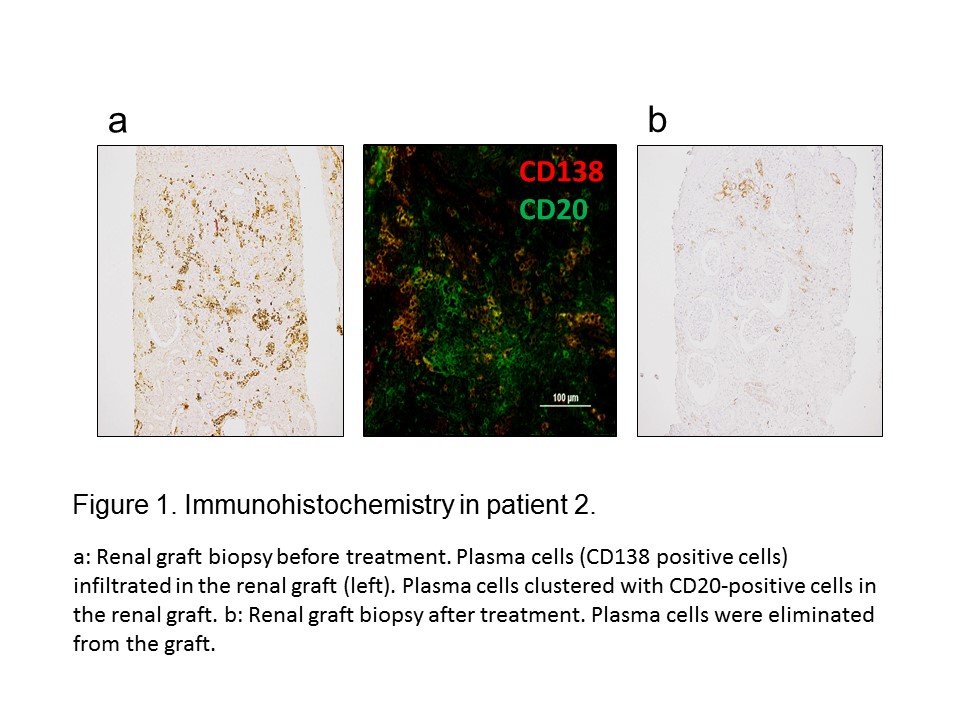
Clinical cases: We report three Japanese patients diagnosed with PCAR accompanied by ABMR. Patient 1 was a 21-year-old man who had elevated serum creatinine 7 years after kidney transplantation. Steroid pulse therapy, rabbit antithymocyte globulin (rATG), plasma exchange (PEX), intravenous immunoglobulin (IVIG), and rituximab therapy were separately administered. Infiltrated plasma cells were persistent in the graft after each treatment, and 2 months later, he was treated with bortezomib, which led to the elimination of plasma cells from the graft. However, his graft function gradually deteriorated. Patient 2 was a 4-year-old girl who had elevated serum creatinine 1 year after kidney transplantation. Graft biopsy showed plasma cells infiltrated and clustered with CD20-positive cells in the renal graft (Figure 1). The combination therapy consisting of steroid, PEX, IVIG, rituximab, and bortezomib was administered. Infiltrated plasma cells were quickly eliminated from the graft (Figure 1), and stabilization of renal graft function has been achieved for 3 years. Patient 3 was a 36-year-old female who was diagnosed as ABMR with PCAR 6 years after kidney transplantation. She received the same therapy as patient 2 and plasma cells dramatically decreased in the graft. Pancytopenia and mild general fatigue were seen in patient 1 after bortezomib administration.
Conclusions: PCAR accompanied by ABMR is associated with a high risk of graft loss after kidney transplantation. Bortezomib, which targets plasma cells, is a potent medical agent that eliminates infiltrated plasma cells from the graft in PCAR. Full therapy, consisting of PEX, IVIG, and rituximab in addition to bortezomib, may be necessary to control PCAR accompanied by ABMR.