
Allograft Trauma in Transplant Recipients. A Case Series
Shafiq Chughtai 1, Shakeeb SK Khan 1, Ahmed AA Ali1.
1Transplant Surgery , Leicester General Hospital , Leicester , United Kingdom
Introduction: We are witnessing an age of violence. There is a parallel increase in transplant activity as well.Kidney and pancrese allografts are placed in illiac fossa making them vulnerable to injury.There are only a handful of case reports describing the results of trauma in transplant recipients.We present our experience of managing traumatic allograft injuries in kidney and kidney pancreas allograft recipient.
Materials and Methods: We describe the outcome of two of our transplant recipients who were exposed to major trauma and managed in different ways.
Case 1: A 46 year old male w ho had undergone a renal transplant 18 years ago, presented following a road traffic accident and was noted to have tenderness at the graft site. Computerised tomographic (CT) scan revealed an isolated grade III lacera
tion of upper pole of transplant kidney with a perinephric haematoma . The patient remained heamodynamically stable and a repeat CT scan on day 3 did not show any increase in the perinephric collection.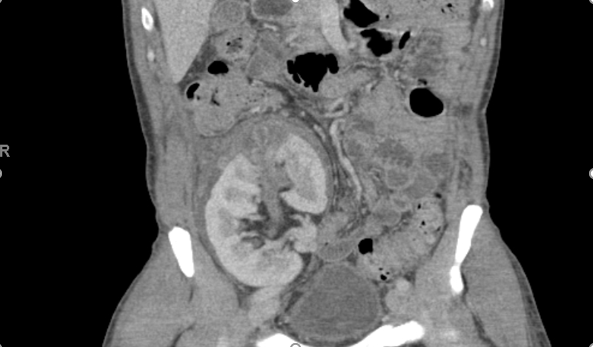 There was an initial increase in his serum creatinine but this subsequently improved and he was discharged on the 6th day. His subsequent clinical course remained uneventful with graft function returning to base line at 6 months follow up.
There was an initial increase in his serum creatinine but this subsequently improved and he was discharged on the 6th day. His subsequent clinical course remained uneventful with graft function returning to base line at 6 months follow up.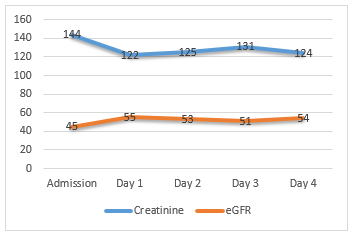
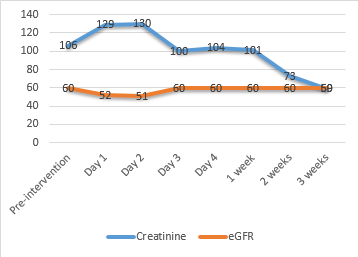
Case 2: A 45 year old male with a simultaneous pancreas kidney transplant done 29 months ago presented following a fall from the second floor. Tenderness was noted over the renal allograft and an urgent CT scan revealed a haematoma with a grade III laceration of the renal graft.Rest of the abdomen and transplanted pancreas were unremarkable.

Patient remained unstable heamodynamically despite adequate resuscitation.After optimization, a follow-up CT scan showed an increase in the size of perinephric haematoma and extravasation of contrast suggestive of an active bleed.It was decided to perform an angiogram and embolization of the bleeding vessel using micro coils. A follow-up doppler scan showed preservation of global perfusion apart from a small avascular area in the upper pole. The patient was discharged with stable graft function on day 10 and no complications identified at 6 months follow up.
Conclusion: Basic principle of resuscitation should be applied in managing traumatic injuries in transplant recipients.Life of the patient takes precedence over the allograft.These cases highlight the importance of close clinical monitoring, serial imaging and the role of interventional radiology in the management of trauma in transplant recipients.

