
Pattern of Glomerular Staining for C4d Immunohistochemistry is Useful for the Diagnosis of Immune Complex Mediated Glomerulonephritis in Renal Allograft Biopsies
Cinthia Drachenberg1, Abdolreza Haririan2, Richard Ugarte2, Charles Cangro2, John C Papadimitriou1.
1Pathology, University of Maryland School of Medicine, Baltimore, MD, United States; 2Medicine, University of Maryland School of Medicine, Baltimore, MD, United States
Introduction: Performance of the C4d stain is required for the adequate evaluation of kidney transplant biopsies (KTBx). Positive C4d staining in the renal peritubular capillaries is very useful for the diagnosis of antibody mediated allograft rejection (AMR) and correlates with poorer graft outcomes. Glomerular C4d staining is common in the chronic phases of AMR but this is not diagnostically useful due to inconsistent distribution and intensity of staining. Deposition of the C4d complement component in immune complex mediated (ICM) glomerulonephritis (GN) is expected but this has not been systematically studied in KTBx.
Materials and Methods: C4d stain (immunohistochemical method) was applied to 2432 consecutive, paraffin embedded KTBx, over a period of 5 years. In KTBx due to abrupt increase in proteinuria or history of GN in the native kidney, immunofluorescence and electron microscopy studies for standard evaluation of GN were also used for diagnosis.
Results and Discussion: In this unselected biopsy cohort, 33 KTBx from 27 patients showed recurrent or primary GN: 12 membranous glomerulopathy (MGN), 4 lupus nephritis (SLE), 9 IgA nephropathy and 8 focal segmental glomerulosclerosis (FSGS), Distinctive and consistent glomerular C4d stainining was noted in patients with MGN with a pattern paralleling the IF and EM findings. SImilarly, in recurrnet SLE, glomerular C4d staining corresponded to the histological lupus Class determined by light microscopy, IF and EM. 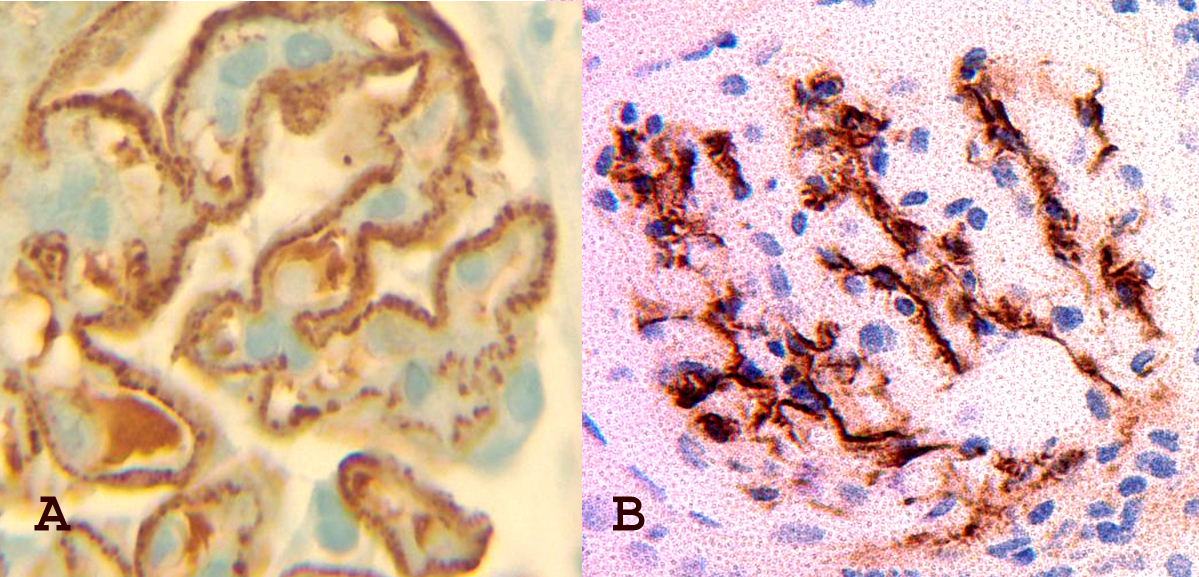 The C4d staining pattern in these GNs was clearly different from that seen in transplant glomerulopathy. C4d staining in IgA nephropathy was inconsistent, mostly mesangial and did not correlate clearly with the strength of IF IgA staining. Only the segmental sclerotic lesions in FSGS were highlighted by the C4d staining in a manner that appeared nonspecific.
The C4d staining pattern in these GNs was clearly different from that seen in transplant glomerulopathy. C4d staining in IgA nephropathy was inconsistent, mostly mesangial and did not correlate clearly with the strength of IF IgA staining. Only the segmental sclerotic lesions in FSGS were highlighted by the C4d staining in a manner that appeared nonspecific.
Conclusions: C4d staining is routinely evaluated in transplant biopsies and this stain consistently highlights immune complex deposits in MGN and SLE. Recognition of this distinctive staining pattern is helpful in the diagnosis of these processes and should prompt complete evaluation with IF and EM if these studies were not initially available. The findings in this study are based on C4d stain evaluation of paraffin embedded tissue sections. Since C4d staining corresponds to the classical pathway of complement activation, similar findings are expected with the IF staining method in fresh frozen tissue sections.

