
Kidney Autotransplantation: Long‑Term Outcomes and Complications. 26-Years Experience in a Tertiary Hospital.
Mercedes Ruiz Hernández1, David D Diaz Pérez1, Vital V Hevia Palacios1, Sara S Álvarez Rodríguez1, Víctor V Díez Nicolás1, Luis L López-Fando1, Cristina C González Gordaliza2, Victoria V Gómez Dos Santos1, Francisco Javier FJ Burgos Revilla1.
1Urology, Ramón y Cajal Hospital, Alcalá University, IRYCIS, Madrid, Spain; 2Radiology, Ramón y Cajal Hospital, Alcalá University, IRYCIS, Madrid, Spain
Introduction & Objectives: Kidney autotransplantation (KAT) is an infrequent procedure in urology. The objective was to analyze indications of KAT, surgical technique, complications and long-term outcomes after 26-year experience at a single institution
Material & Methods: A retrospective observational study of patients who underwent KAT at our institution (January 1990–December 2016) was carried out. Data collected included indications, surgical technique, complications (Clavien–Dindo), hospital stay and long-term outcomes. Follow-up data were obtained through visits including anamnesis, physical examination, laboratory analysis including serum creatinine and finally imaging and functional tests: Doppler ultrasound, contrast-enhanced ultrasonography (CEUS) and CT scan. (Fig.1)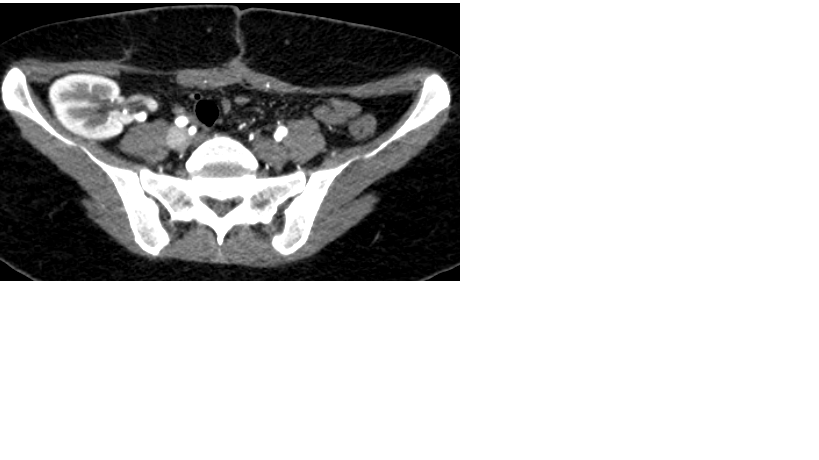
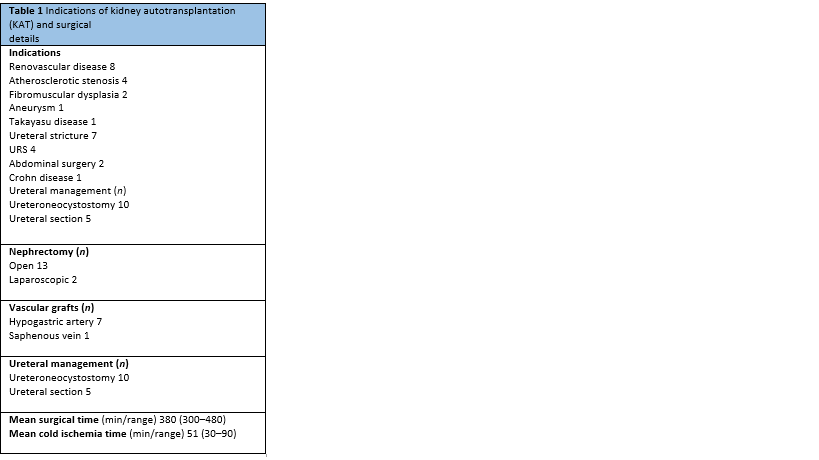
Results: Fifteen patients underwent a KAT, with a mean age of 41 years (range 34–59). Indications were vascular abnormalities in 8 cases and ureteral injury in 7. The cases of vascular disease were: 4 atherosclerotic stenosis, 2 fibromuscular dysplasia, 1 Takayasu’s disease stenosis and 1 renal artery aneurysm. The cases of ureteral injuries were: 6 iatrogenic lesions (4 after ureterorenoscopy, 1 after segmental colectomy and 1 after laparotomy for ectopic pregnancy) and 1 secondary to Crohn’s disease.
Nephrectomy was performed through laparoscopy in 2 cases (13.3%) and open in 13 (86.7%). Vascular grafts were used in 8 patients (7 from hypogastoric artery and 1 from saphenous vein), and ureteral reimplantation was performed in 11 cases. Whenever possible, ureteral reimplantation was avoided to preserve natural draining in the bladder trigone (Fig.2). When it was not possible a stented tunnelled extravesical ureteroneocystostomy was chosen (Barry technique).
Mean surgical time was 380 min (range 300–480).Mean cold ischemia time was 51 min (range 30–90) and mean hospital stay was 9.1 days (range 3–20). (Table1)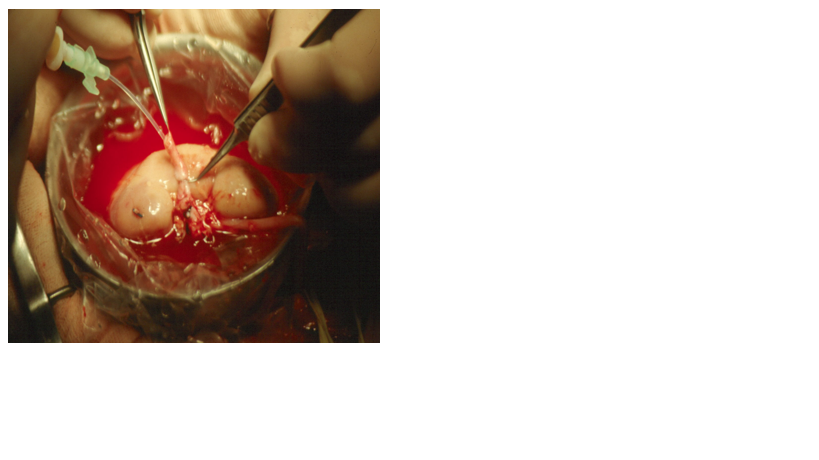
Seven patients (46.7%) developed postoperative complications: 5 Clavien I (urinary tract infection, fever unknown origin, 3 acute renal failure), 1 Clavien II (surgical site abscess treated with antibiotics) and 1 Clavien IVa (renal vein thrombosis requiring nephrectomy).
After a mean follow-up of 73.1 months (range 7–312), mean serum creatinine level was 1.4 mg/dl (range 0.7–1.6) and 80% of the patients have a functioning graft (3 kidney losses: 1 early renal vein thrombosis and 2 chronic kidney disease).(Table2)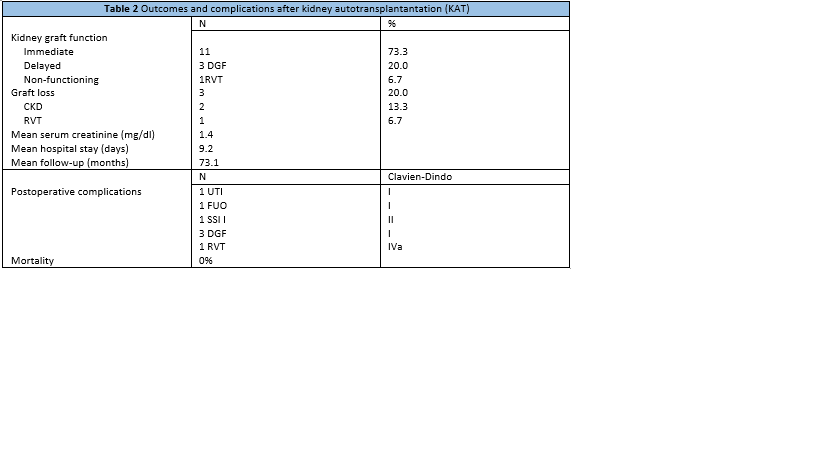
Conclusions: Kidney autotransplantation is an effective treatment for complex ureteral lesions and kidney vascular abnormalities, with good results even in long term. Surgical complications are quite frequent, but most of them are minor (Clavien I–II) and do not compromise kidney survival. As a challenging surgery, sometimes requiring vascular grafts, it should be performed by experienced kidney transplant surgeons.

