
Long-term Follow-up after Short Renal Vein Repair Procedure in Kidney Transplantation
Sinh Tran1, Ngoc Thu T. Du1.
1Urology, Cho Ray Hospital, Ho Chi Minh City, Viet Nam
Introduction and Objective: In this clinical serial, we would like to introduce a surgical technique for kidney transplantation (KTx) from living donor; we call the vessel disposition procedure (DVP), with long-term follow-up results.
Methods: A serial case study with control group. The patients (pts) underwent KTx at Cho Ray Hospital (CRH) from 1998 to 2011; they were followed up to year 2016.The pts devided in 2 groups: the VP group: the renal graft (RG) mainly were right kidney removed by live donor laparoscopic nephrectomy (LDLN), with short vein (≤20mm). The VDP applied on the RG (renal DVP): dissection, prolongation and moving on the renal vessel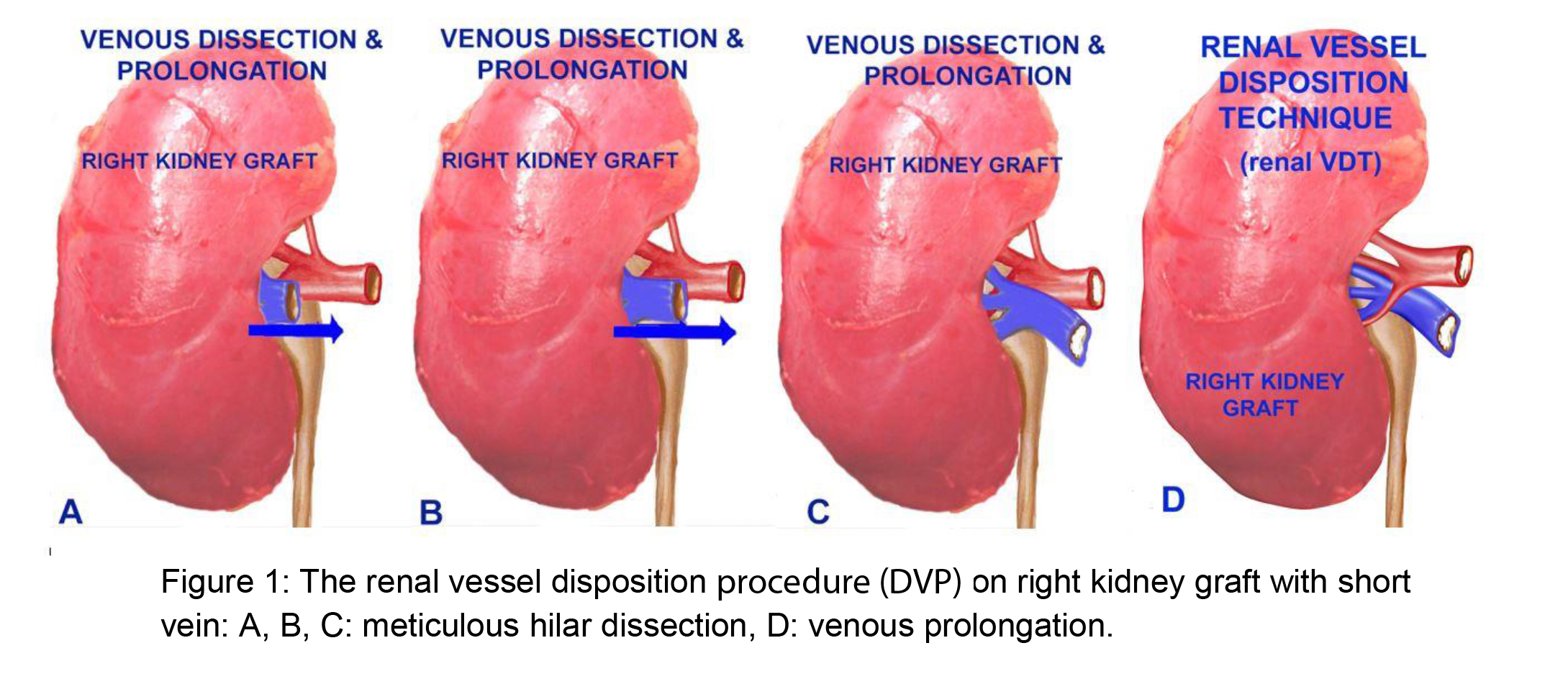 on iliac vessels of the pts (iliac DVP): dissection and moving of right external iliac vein (RIV) to the right side of the right external iliac artery (RIA
on iliac vessels of the pts (iliac DVP): dissection and moving of right external iliac vein (RIV) to the right side of the right external iliac artery (RIA 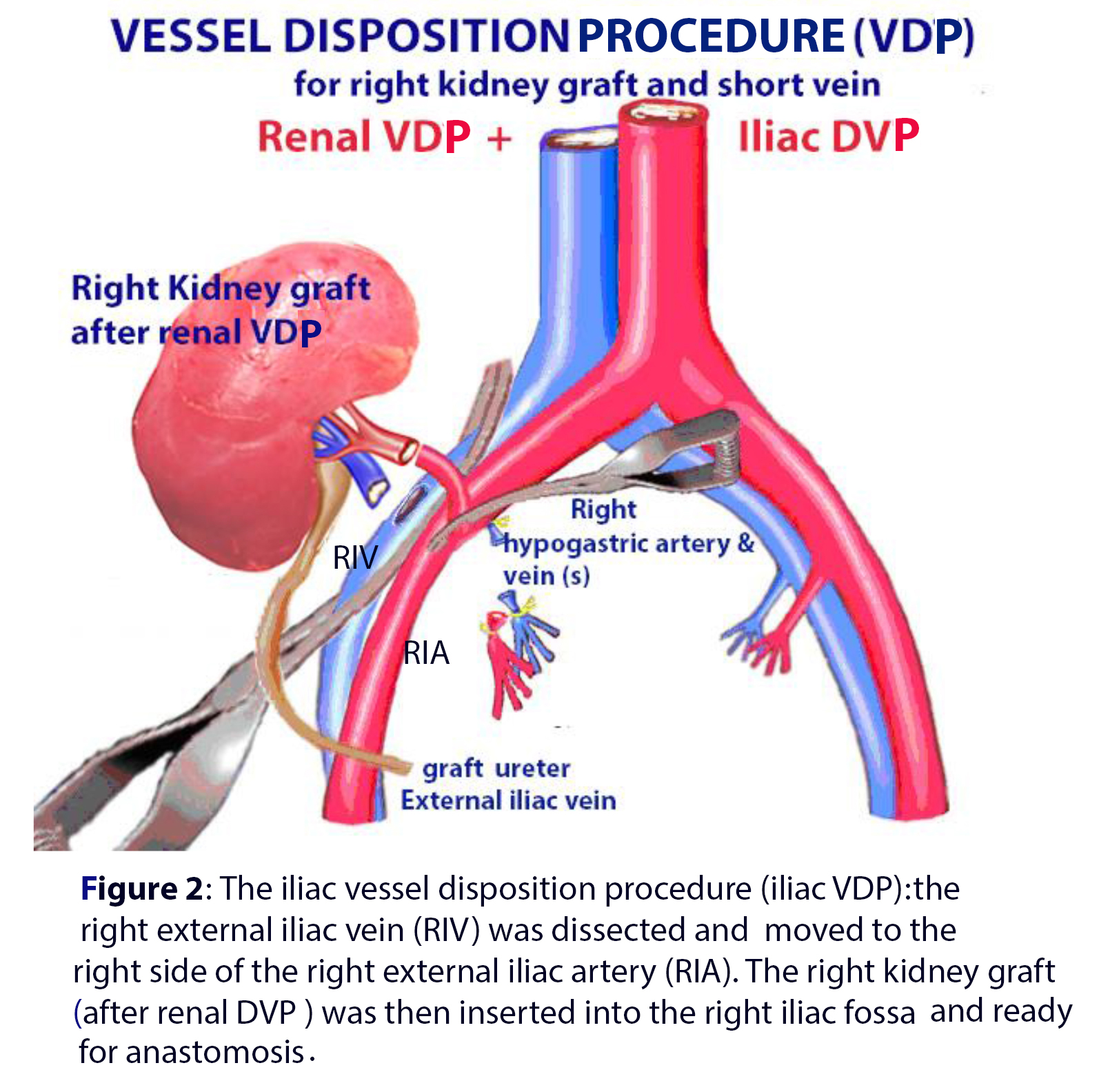 the kidney then was transplanted on the right iliac fossa (RIF). The control group: the RG with long enough vein (>20mm), the kidney transplanted as classic surgical technique on RIF. The renal graft vein was sutured “end to side” with the iliac vein; renal artery sutured to RIA or to the hypogastric artery. The surgical team was the same for both groups. Postoperative following up (FU) were vascular perfusion by Doppler ultrasound and kidney function (serum creatinine).
the kidney then was transplanted on the right iliac fossa (RIF). The control group: the RG with long enough vein (>20mm), the kidney transplanted as classic surgical technique on RIF. The renal graft vein was sutured “end to side” with the iliac vein; renal artery sutured to RIA or to the hypogastric artery. The surgical team was the same for both groups. Postoperative following up (FU) were vascular perfusion by Doppler ultrasound and kidney function (serum creatinine).
Results: There were 201 pts., 130 males (64.7%) and 71 females (35.3%). Average age is 33.56 ± 8.62 year old (yo), range [15 to 61 yo]. DVP group: there were: 63/201 pts (31.34%). These 63 pts, the RG were transplanted on RIF, by the right Gibson incision. But only 50/63 RG were the right kidney (79.37%), applied totally “renal DVP” (including prolonging and moving of renal vein) and 13/63 pts were the left KG (20.63%) applied partially “renal DVP’ (dissecting and prolonging of renal vein). The control group: there were 138/201 pts (68.66%) pts, the RG with the long veins enough (>20 mm) were normally transplanted on RIF. The average FU time was 8.0±3.44 years (group A) and 8.79±4.07 years (group B). The vascularization of the renal vein and renal artery was postoperatively followed-up by Doppler ultrasound showed not significantly different between two groups; no relation of vascular function and kidney function by following up with serum creatinine on both two groups. There wasn’t any other surgical vascular complication during FU time.
Conclusions: During the long-term following-up, all the pts of VDT group was satisfactory, like the control group. The KTx from living donor with short vein could be repaired easily and safety by the DVP. The RG could be not only the right kidney but may be the left kidney due to LDLN.
The new conception is the right RG could be safety transplanted on the RIF with applying the DVP, as the left RG could be transplanted on the right RIF. With the DVP we could avoid a venous reconstruction and avoid its surgical complication.
Donors, recipients and staffs of Cho Ray Hospital.

