
Safety and Efficacy of Robot-Assisted Kidney Transplantation
Harkiran Sran1, Ben Lindsey1, Colin Forman1, Peter Dupont2, Ravi Barod3, Neal Banga1.
1Department of Renal Transplant Surgery, Royal Free London NHS Foundation Trust, London, United Kingdom; 2Department of Nephrology, Royal Free London NHS Foundation Trust, London, United Kingdom; 3Department of Urology, Royal Free London NHS Foundation Trust, London, United Kingdom
Introduction: Robot-assisted kidney transplantation (RAKT) is thought to offer the benefits of faster recovery and fewer wound complications than open kidney transplantation (OKT), and may ultimately improve access to transplantation for obese patients. Our centre began its RAKT programme one year ago, and currently has the largest series in the UK. We aimed to evaluate the safety and efficacy of this new procedure.
Methods: Data from RAKT recipients was compared in a 1:2 ratio to a control group of consecutive OKT recipients. All transplants were performed by the same surgeon. The primary outcome measure was graft function at 3 and 6 months post-transplantation. Secondary outcomes were implantation time, operative time, wound infection rate, return to theatre, and length of stay (LOS).
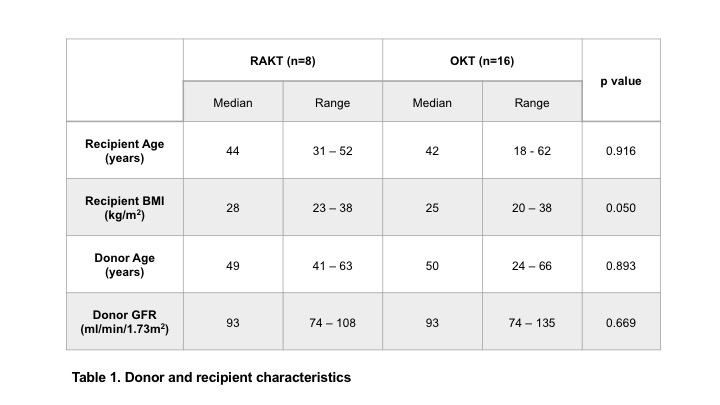
Results: We have performed RAKT in 8 patients. All patients received an ABO-compatible live donor graft with single vessels, with no significant differences in donor or recipient characteristics between the groups (table 1). Implantation and operative times were significantly longer in the RAKT group (table 2). All grafts experienced primary function, with no difference between the groups in eGFR at 3 months (62 vs 57mls/min, p=0.76) or at 6 months (57 vs 57mls/min, p=0.95) post-transplant. One patient in the OKT group underwent re-operation for bleeding. There were no wound infections, and median LOS was 6 days in both groups. At the time of writing, graft and patient survival in both groups is 100%.
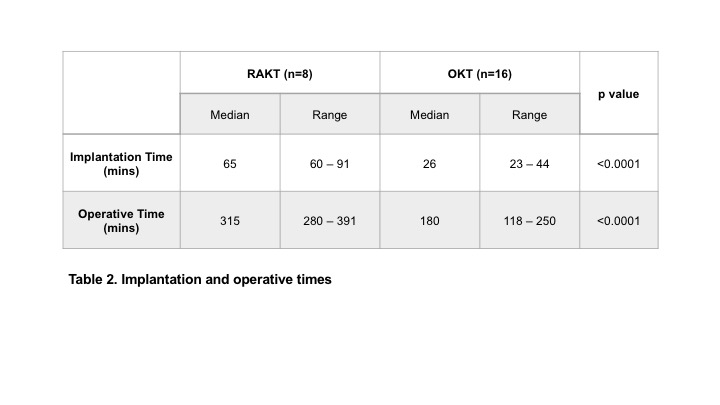
Conclusions: RAKT is a technically challenging procedure with a steep learning curve, resulting in longer implantation and operative times. Close co-operation between transplant surgeons, urologists and anaesthetists, specialist training and mentorship in robotic surgery, and the use of intracorporeal ice for graft cooling allows safe progress through this learning curve. This results in equivalent graft outcomes - even in initial cases - to those from OKT.

