

Mechanisms of Vascularized Bone Marrow Graft Protection of Vascularized Composite Allografts
Evan B Buckingham1, Nicole M Shockcor1, Wessam Hassanein1, Cinthia Drachenberg1, Arthur J Nam1, Stephen T Bartlett1, Rolf N Barth1.
1Surgery, University of Maryland School of Medicine, Baltimore, MD, United States
Background: Co-transplantation of vascularized bone marrow (VBM) promotes vascularized composite allograft (VCA) survival with standard immunosuppression in a non-human primate (NHP) model. We investigated mechanisms of immunomodulation by comparing VCA survival following donor bone marrow cell (BMC) infusion, donor and recipient conditioning strategies, and heterotopic VBM allografts to historical groups.
Methods: Groups of 3-4 NHP received facial subunit VCA and immunosuppression of tacrolimus (Tac) and mycophenolate mofetil (MMF). Comparative groups, VCA+VBM (n=4) and VCA (no VBM, n=3) were from historical cohorts (Group 1 and 2, respectively). Group 3 received VCA without VBM and transfused donor BMC at 20x 106 cells/kg on d 1. Group 4 received VCA+VBM following donor mandible irradiation (1.5 Gy) on d -1, while Group 5 received irradiated donor mandible followed by BMC transfusion on d 1. Group 6 underwent co-transplantation of heterotopic VBM and VCA without VBM. Group 7 received VCA+VBM after donor T cell depletion with anti-thymocyte globulin (ATGAM, 50 mg/kg) on days -2, and -1. An additional dose of ATGAM was given on d 0 if CD3+ cells remained >50/mm3. Group 8 recipients received ATGAM depletion as above, VCA+VBM, and a 21-d steroid taper. Banff classification was determined by histopathologic analysis. Chimerism was assessed by flow cytometry from peripheral blood and sampled tissues.
Results: VCA + VBM treated with Tac/MMF demonstrated prolonged graft survival and rejected only after immunosuppression was withdrawn compared to Groups 2-8 (mean survival 348d vs 36d).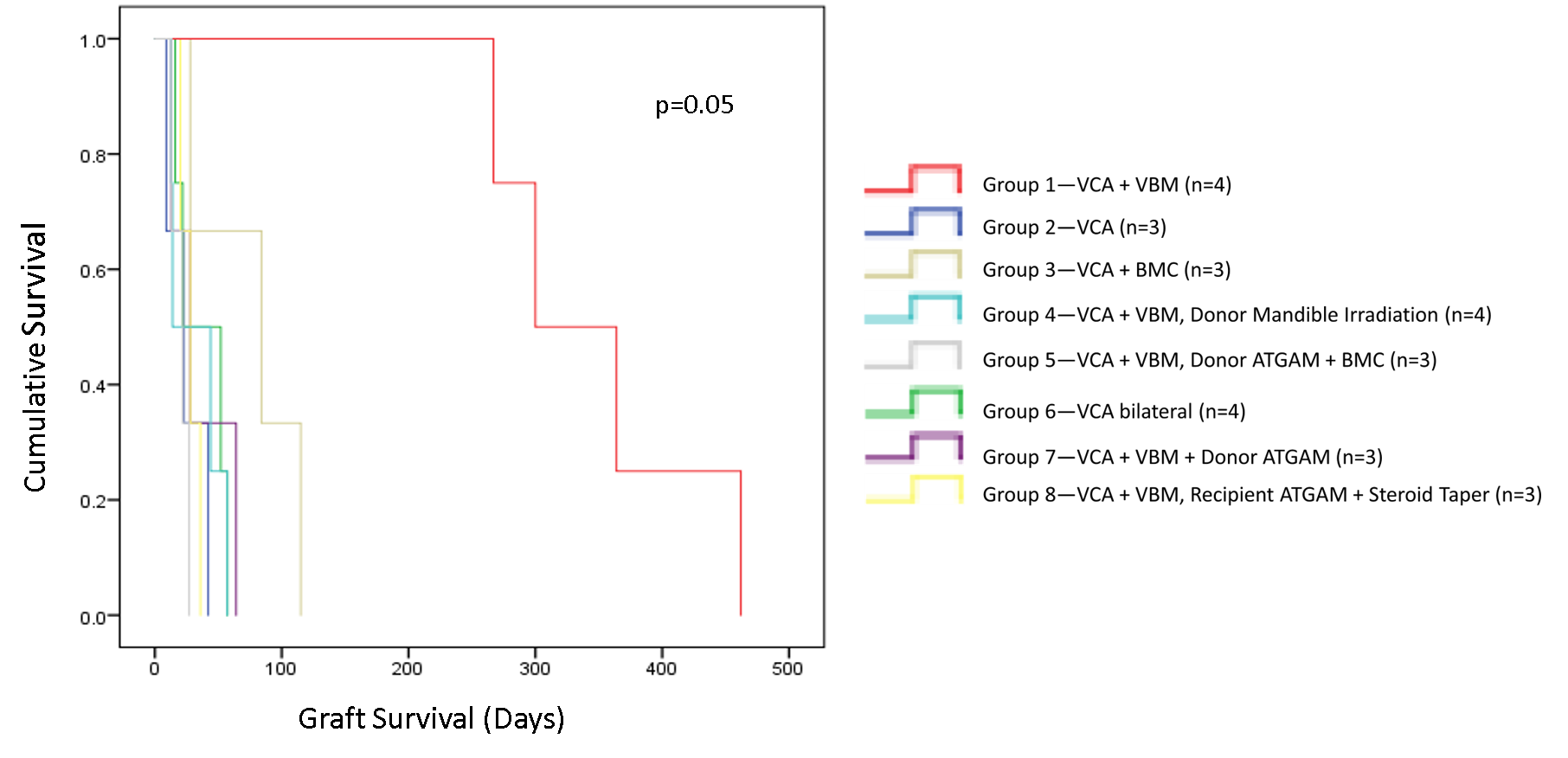 This effect was statistically significant (p=0.05). Endpoints were met secondary to Banff IV rejection and malignancy. Macrochimerism was present only in Group 1; remaining groups demonstrated only transient microchimerism.
This effect was statistically significant (p=0.05). Endpoints were met secondary to Banff IV rejection and malignancy. Macrochimerism was present only in Group 1; remaining groups demonstrated only transient microchimerism.
Discussion: The immunologic advantage of VBM prolonging VCA graft survival is contingent on proximity of the VBM to the VCA allograft. Donor conditioning nullifies this benefit and it is not reconstituted by transfusion of donor BMC. Recipient T cell depletion mirrors the early graft loss observed with donor T cell depletion.
Conclusion: Our data elucidate a mechanism for VCA graft survival that is mediated by locally acting, radiosensitive T cell populations in both donor and recipient and is dependent on the unique immunologic and structural niche of VBM.
Astellas Pharma, Inc .

