Outcomes from Brain Death Donors with Cardiac Arrest Accepted for Pancreas Transplantation
Pedro Ventura-Aguiar1, Joana Ferrer2, David Paredes3, Camino Rodriguez3, Constantino Fontdevilla2, Enric Esmatjes4, Juan Carlos Garcia-Valdecasas2, Federico Oppenheimer1, Fritz Diekmann1, Maria Jose Ricart1.
1Nephrology and Kidney Transplant Department, Hospital Clinic, Barcelona, Spain; 2Hepatobiliopancreatic and Liver Transplant Department, Hospital Clinic, Barcelona, Spain; 3Organ Transplantation Coordination Department, Hospital Clinic, Barcelona, Spain; 4Diabetes Unit, Department of Endocrinology and Nutrition, Hospital Clinic, Barcelona, Spain
Donor selection has a major impact on pancreas transplantation. Cardiac arrest and hypoxemia produce an insult to endothelial cell and may increase the risk of platelet adhesion and thrombosis. Results from donors after cardiac death report good outcomes with functional warm ischemia times up to 48minutes. We proposed to evaluate the effect of cardiac arrest from donors after brain-death (cDBD) on pancreas transplant outcomes.
We conducted a retrospective analysis on all pancreas transplant recipients at our center from 2000 to 2016 (n=359). A total of 49 cDBD were accepted for transplantation (median arrest time of 5.0 minutes [IQR 2.0-13.5]). Expectedly, cerebral anoxia as COD was most frequent and P-PASS higher (15.6 vs 16.9) in cDBD group when compared to the remaining DBD donors (sDBD). Donor demographics, PDRI and all P-PASS sub-categories (excluding cardiac arrest), biochemical, graft perfusion solution, and cold ischemia time, were similar between groups.
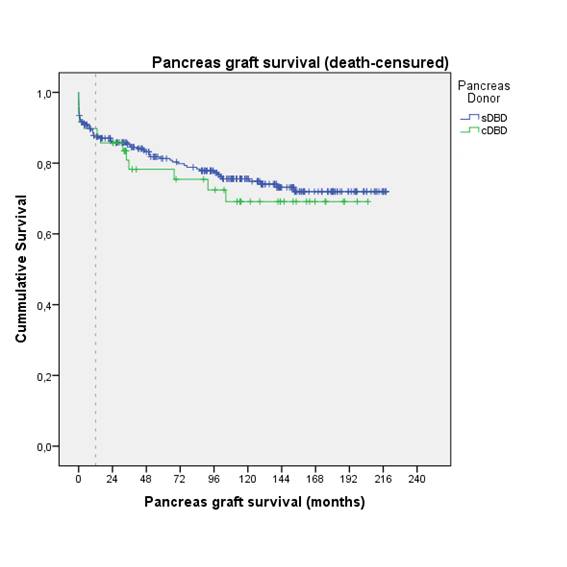
Estimated graft survival was similar between both groups (log-rank p=0.576). Overall, cardiac arrest did not increase the risk of graft loss due to technique failure (p>.05). On univariate analysis, the duration of cardiac arrest was associated with an increased risk of technique failure (HR 1.16 [95% CI 1.05-1.27]). The ROC curve for cardiac arrest duration to discriminate technique failure had an AUC of 0.94 (95% CI 0.87-1.0). With a cutoff of 15minutes, cardiac arrest had an 100% sensitivity and 83.7% specificity.
In conclusion, cDBD donors with a cardiac arrest inferior to 15minutes may be suitable for pancreas transplantation without increasing technique failure risk.