
Helong Dai, P.R. China has been granted the TTS Young Investigator Scientific Award
Distal Abdominal Aorta Could Serve as an Outflow Tract for en Bloc Kidney Transplantation from Infant Donors with Extremely Low Body Weight
Helong Dai1,2, Longkai Peng1, Fenghua Peng1, Gongbin Lan1, Yu Wang1, Jingjing Chen1, Lei Liu1, Chen Gao1, Yong Guo1, Chunhua Fang1, Manhua Nie1, Wang Long 1, Shaojie Yu1.
1Department of Urological Organ Transplantation, The Second Xiangya Hospital of Central South University, Changsha, P.R. China; 2Department of Surgery, Thomas E. Starzl Transplantation Institute, University of Pittsburgh School of Medicine, Pittsburgh , PA, United States
Introduction: Pediatric kidney donors are underutilized due to high risk of postoperative thrombosis, urinary complications, acute rejection, delayed graft function (DGF) and the development of hyper-filtration injury. To address these problems, we develop a novel en bloc kidney transplantation by using distal abdominal aorta as an outflow tract.
Methods: Briefly, 8 cases of en bloc kidneys from deceased infant donors younger than 5 months with low body weight (1.9-4.9 kg) were transplanted into 4 pediatrics and 4 adults. Donor's common iliac artery or external iliac artery was anastomosed to recipient's distal external iliac artery (cases 1-4) or inferior epigastric artery (cases 5-8) respectively as an outflow tract (Figure 1).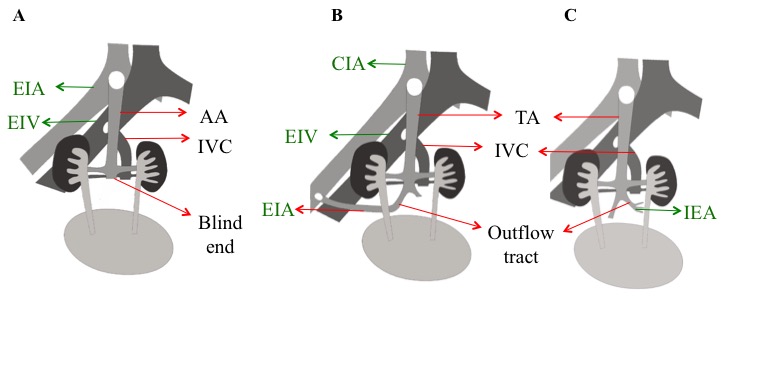 Recipients received Basiliximab or antithymocyte globulin as induction therapy followed by Tacrolimus, Mycophenolate Mofetil, and prednisone but without prophylactic anticoagulation.
Recipients received Basiliximab or antithymocyte globulin as induction therapy followed by Tacrolimus, Mycophenolate Mofetil, and prednisone but without prophylactic anticoagulation.
Results: Delayed graft function was observed in 1 patient but was reversed at 90 days post-transplant. Two patients had urine leakage, which was cured by conservative treatments. Two recipients developed lung infection that was eventually cleared. However, none of them showed vascular thrombosis post-transplant. Outflow tracts were not seen in all pediatric recipients (Figure 2A), but were seen in all except one of the adult recipients by CTA scanning at 1-month post-transplant (Figure 2B). One of adult recipient's outflow tracts was still maintained at 1-year post-transplant (Figure 2C).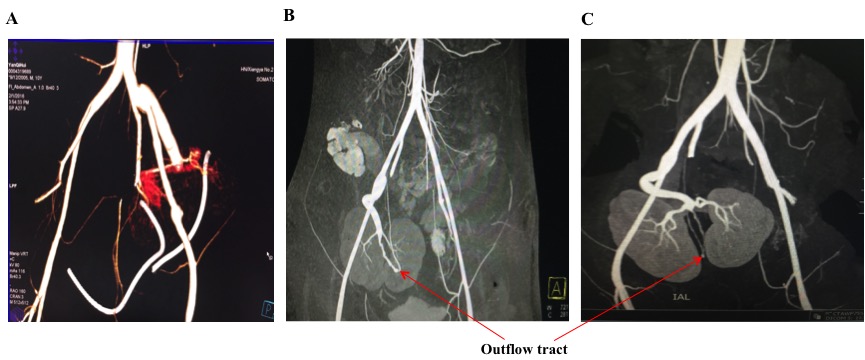 Currently all patients are well with normal serum creatinine values at 1-1.5 years follow-up (Figure 3).
Currently all patients are well with normal serum creatinine values at 1-1.5 years follow-up (Figure 3).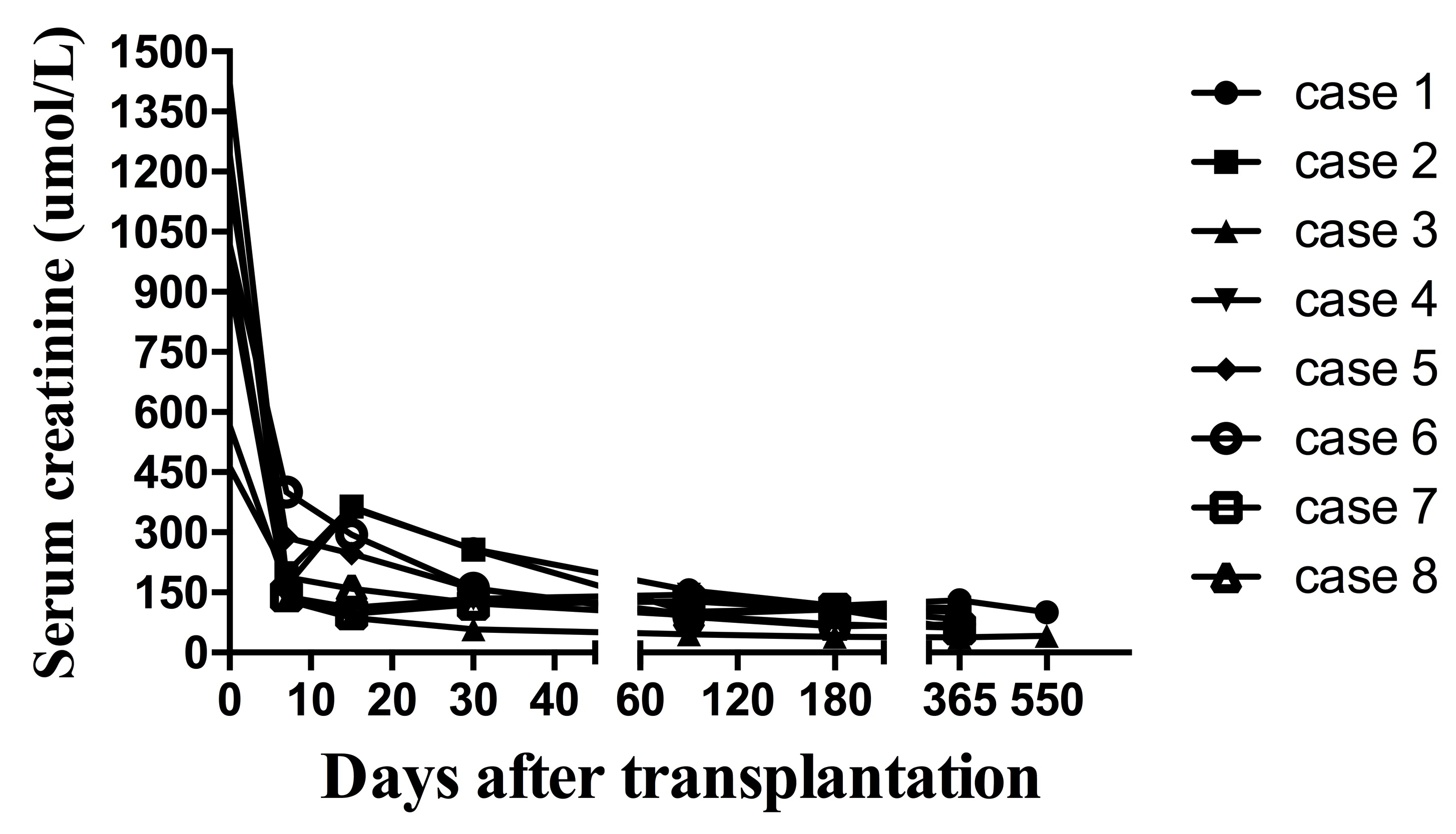
Conclusion: This technique provides a solution to the challenges of using infant donors with extremely low body weight even in the absence of anticoagulants. Therefore, using infant en bloc kidneys with an outflow tract should be encouraged to address the problem of organ shortage. The safety and efficacy of this novel technique, as well as its mechanism still require a long-term follow-up of more cases in the future.

