
Antibody Mediated Rejection Due to De-Novo DSA causing Venous Thrombosis of Pancreas Allograft – A Case Report
Kunal Yadav1, Pamela Kimball1, Laura Warmke3, Gaurav Gupta2, Marlon Levy1, Adrian Cotterell1.
1Department of Surgery, Virginia Commonwealth University, Richmond, VA, United States; 2Department of Internal Medicine, Virginia Commonwealth University, Richmond, VA, United States; 3Department of Pathology, Virginia Commonwealth University, Richmond, VA, United States
A 34 year old female with chronic kidney disease secondary to DM-i underwent an HLA identical living donor kidney transplant with a weakly positive flow cytometric crossmatch (FCXM), but without any donor specific antibody (DSA) [Table1]. Crossmatch became progressively more positive with time, but without detectable DSA. Tests to detect non-HLA antibody and autoantibody were negative. Allograft function was good, protocol biopsies did not show any rejection. She later received a pancreas allograft, again with a weakly positive FCXM, without DSA. The pancreas functioned well until about 6 weeks posttransplant when she developed hyperglycemia. Cross-sectional imaging demonstrated non-enhancing pancreas allograft with new vein thrombosis. She underwent transplant pancreatectomy of the non-viable, necrotic graft. Pathology demonstrated massive parenchymal necrosis, numerous intravascular thrombi, inflammation of the viable pancreas with C4d deposition in the vessels.
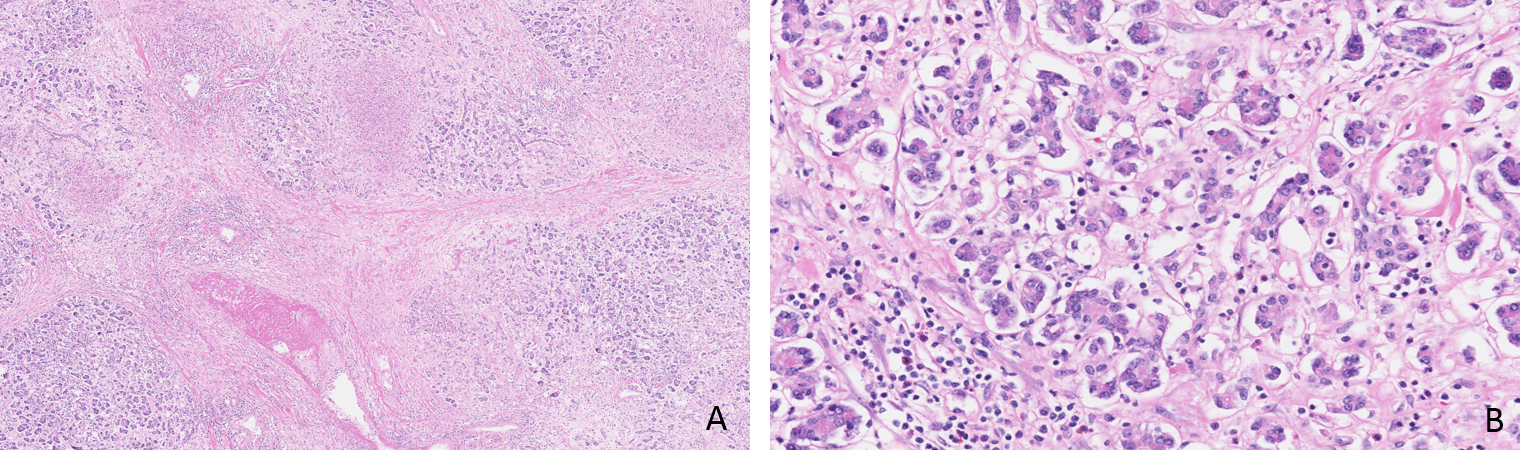
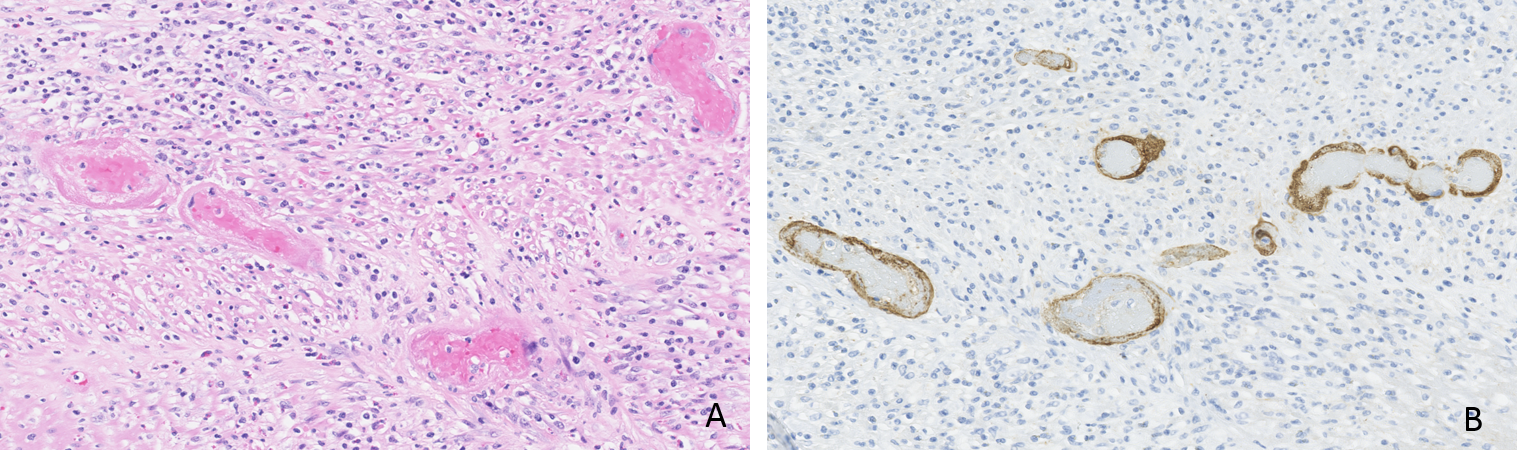
She had also developed several de-novo class-I DSAs at this time [Table2]. This is consistent with severe acute antibody mediated rejection (AMR) of the pancreas leading to venous thrombosis and graft necrosis. Despite extensive testing, we were not able to identify a causative antibody for the initial positive FCXMs or its role in the eventual rejection of the pancreas allograft.
Table 1. CDCXM and FCXM results with brother (kidney donor), self and tested pancreas donors
MCS – Mean Channel shift, KTx – Kidney transplant, N- negative, P – positive, PTx – Pancreas transplant
(A channel shift of ≥ 40 is considered positive for both T and B-cell FCXMs at our institution)
|
Date |
Donor | CDC-T cell | CDC-B cell | FCXM-T cell (MCS) | FCXM-B cell (MCS) |
| Pre-KTx | Brother | N | N | 92 | 77 |
| Pre-KTx | Self | N | N | - | - |
| KTx +14 mo | Panc offer | N | N | 61 | 193 |
| Retest brother | N | N | 310 | 257 | |
| KTx+37 mo | Retest brother | P | P | 203 | 225 |
| KTx+38 mo (PTx) | Panc donor | N | N | N | 76 |
| PTx+1 mo | Panc donor | N | N | 91 | 100 |
| PTx+1.5 mo | Panc donor | P | P | 234 | 82 |
Table 2. Donor specific antibodies to the pancreas donor at the time of graft failure (MFI – Mean fluorescence index)
| Specificty | MFI |
| A23:01 | 6677 |
| B44:03 | 4130 |
| B37:01 | 3669 |
| C05:01 | 1087 |

