Utility of Multi Locus Sequence Typing (MLST) in the Investigation of a Cluster of Candida albicans Infection in Recipients of Solid Organs from a Common Donor
Ines Ushiro-Lumb1,2, Andrew Borman3, Elizabeth Johnson3, Tyrone Pitt1, Donna MacCallum4.
1Microbiology Services, National Health Service Blood and Transplant, London, United Kingdom; 2National Infection Service, Public Health England, London, United Kingdom; 3Mycology Reference Laboratory, Public Health England, Bristol, United Kingdom; 4Aberdeen Fungal Group, University of Aberdeen, Aberdeen, United Kingdom
Introduction: Invasive candidiasis can be of endogenous or exogenous origin and is a cause of significant morbidity and mortality in solid organ transplant recipients. Contamination of the preservation fluid at the point of organ retrieval is a commonly proposed source.
MLST is a highly discriminatory method based on the analysis of single nucleotide polymorphisms within the sequences of seven PCR-generated regions of housekeeping genes, which are combined to produce diploid sequence types (DST). This technique has been used to analyse isolates from three solid organ recipients.
Material and Methods: A 21 year old woman who died of hypoxic brain injury secondary to hanging became a donor of tissues and organs. The right kidney recipient lost the graft 26 days post-transplant (PT) due to Candida arteritis. Blood cultures and a perinephric blood clot grew C. albicans; preservation fluid (PF) yielded no growth. The left kidney and pancreas recipient received anti-fungal prophylaxis following isolation of C. albicans from the PF and did not develop complications. The liver recipient succumbed to a ruptured pseudoaneurysm of the aortic conduit on PT day +23; C. albicans grew from the vascular tissue. Another liver recipient in the same transplant unit had recently died of the same complications from Candida infection. Isolates from all 3 recipients were analysed by MLST.
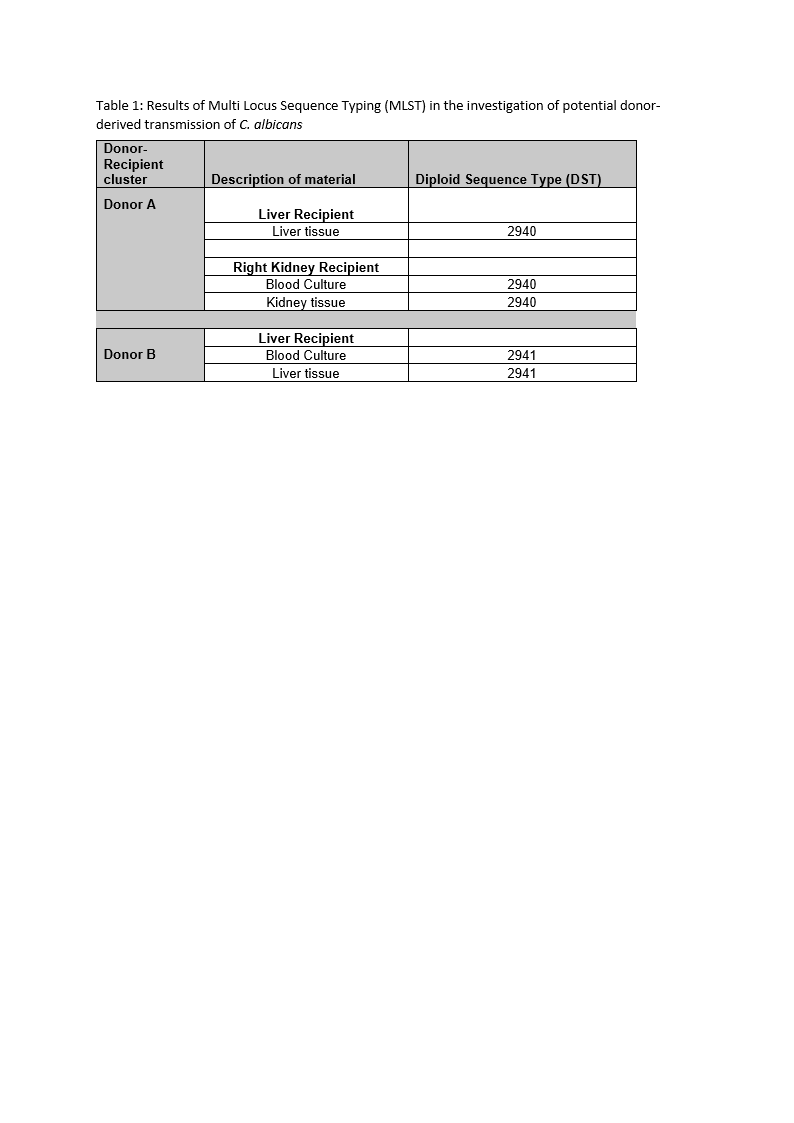
Results: Three isolates from recipients linked to donor A were genetically indistinguishable from each other and of the same novel DST; the other two isolates were also identical but of a different novel DST (Table 1). These two DSTs differed at 5 of 7 loci.
Discussion and Conclusion: Overall PF yeast contamination rates in abdominal organ retrieval vary between 0.4 to 4%, with C. albicans being the most common species found. Imputability of an infection source is not always possible and availability of isolates for analysis and access to appropriate techniques can be limiting factors. Inclusion of unrelated, control samples adds strength to the analysis and should be incorporated whenever possible. Contamination from the GI tract of a colonised donor is the most likely explanation for recipient infection in cluster A. In the absence of an isolate from the donor, our results do not unequivocally confirm the origin of the strain of C. albicans; however, the strain type isolated from cluster A recipients had not been previously described, indicating that it is not a common strain type and highly unlikely to have arisen in the two organ recipients by chance. In our series, the use of MLST provided strong supporting evidence for a common source of C. albicans for the right kidney and liver recipients linked to a common organ donor.