
The MADELEINE (coMbined tAcrolimus anD EveroLimus Early ImmuNosupprEssion) Study: CMV and BKV Infections Over the First 6 Months Post-Transplant.
Thomas Jouve1,3, Raphaele Germi3,4, Johan Noble1,3, Bénédicte Janbon1, Gaëlle Fiard2,3, Paolo Malvezzi1, Lionel Rostaing1,3.
1Nephrology, dialysis, apheresis and transplantation, Grenoble University Hospital, Grenoble, France; 2Urology and kidney transplantation, Grenoble University Hospital, Grenoble, France; 3Medical sciences, Grenoble University, Grenoble, France; 4Virology department, Grenoble University Hospital, Grenoble, France
Cytomegalovirus (CMV) and BK Virus (BKV) infections are frequent complications of the immunosuppression regimen after kidney transplantation. A combined regimen of calcineurin inhibitor (CNI) and mTOR inhibitors (mTORi) reduces the rate of CMV and BKV infections after transplantation. However, there is a lack of data concerning antithymocytes globulins induced patients. We report on our experience with early tacrolimus and everolimus, the MADELEINE (coMbined tAcrolimus anD EveroLimus Early ImmuNosupprEssion) study.
In this study, we prospectively enrolled new kidney transplant recipients at our center between july of 2016 and july of 2017. Inclusion criteria were non-sensitized, ABO compatible, first time kidney transplant recipient, age 18 or older, either recipient CMV positive, or CMV negative for both the donor and the recipient. Patients received an induction with antithymocyte globulins, steroids and tacrolimus together with everolimus from day 1 post-transplantation. Steroids were maintained over at least the first 3 months, then depending on a systematic kidney biopsy at month 3. Targeted trough levels over the first month were 5-7 µg/l for tacrolimus and 4-6 µg/l for everolimus, then 4-5 for tacrolimus and 5-7 for everolimus. We did not use CMV prophylaxis.
We monitored CMV and BKV blood PCR preemptively over the first 6 months, at month 0, 1, and 3 and for any suspicion of infection. We defined a viral infection as a positive PCR > 1000 (3 log) copies/ml.
We included 58 consecutive patients. Trough concentrations for tacrolimus and everolimus are represented on figure 1.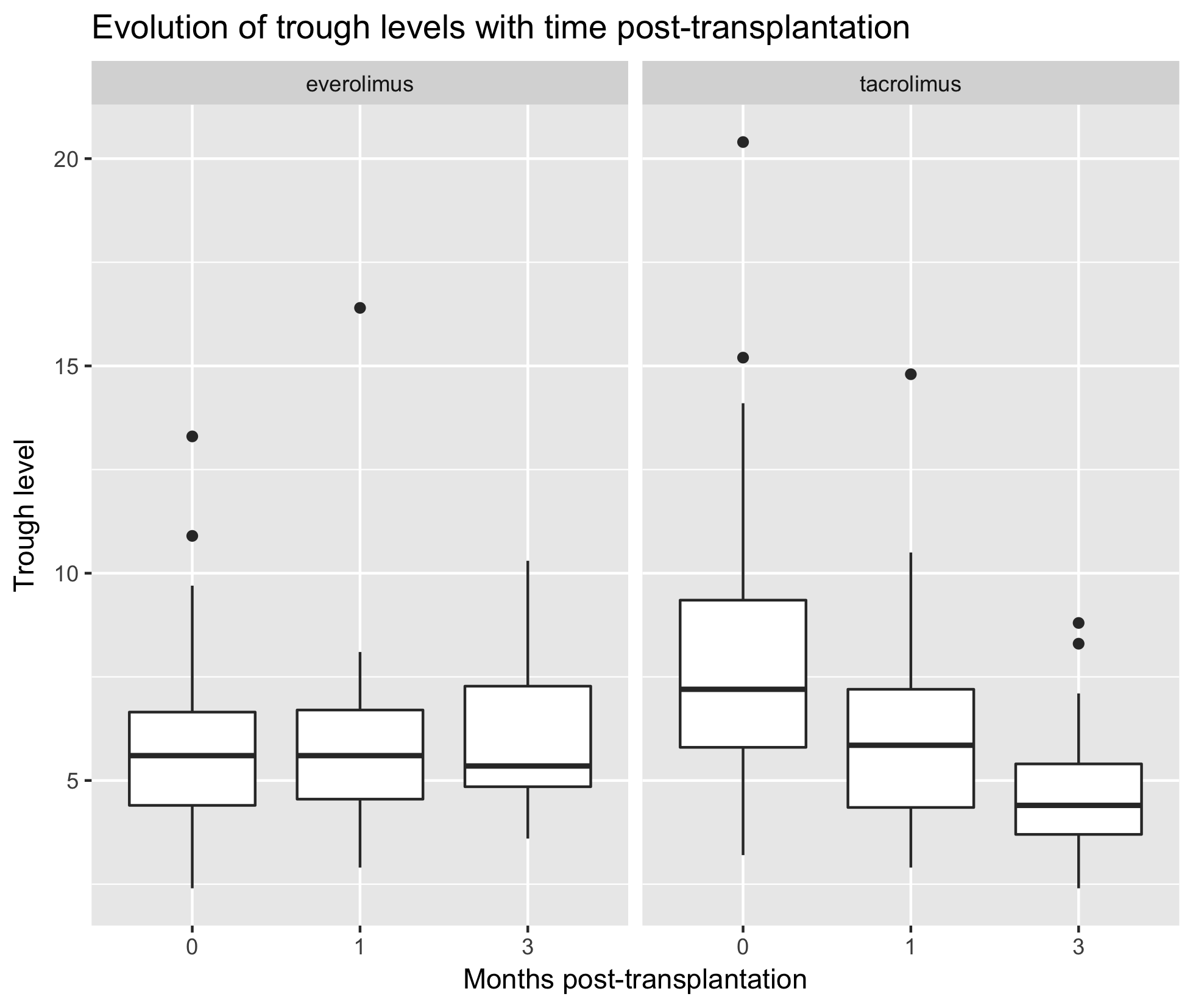 The rate of CMV infections was 8/58 (13.8%), with a mean time time between transplantation and infection of 72 (min=30, max=214) days. The rate of BKV infections was 3/58 (5.1%), with a mean time between transplantation and infection of 91 (min=33, max=177) days.
The rate of CMV infections was 8/58 (13.8%), with a mean time time between transplantation and infection of 72 (min=30, max=214) days. The rate of BKV infections was 3/58 (5.1%), with a mean time between transplantation and infection of 91 (min=33, max=177) days.
Compared to a 10% rate of CMV infections reported in the literature, it seems that using tacrolimus together with everolimus is efficient in preventing CMV and BKV infections, even in antithymocytes globulines induced patients.

