
Impact of Different Dynamic Preservation Strategies on Early Renal Function and Physical Machine Perfusion Parameters in a Porcine DCD Auto-Transplant Model
Tom Darius1, Pierre Gianello2, Antoine Buemi1, Martine de Meyer1, Michel Mourad1.
1Surgery and Abdominal Transplant Unit, University Clinics Saint Luc, Brussels, Belgium; 2Pôle de Chirurgie Expérimentale et Transplantation, Université catholique de Louvain, Brussels, Belgium
Introduction:Continuous and end ischemic preservation strategies (hypothermic machine perfusion (HMP) and normothermic perfusion (NP)) have demonstrated improved early graft function compared to static cold storage (SCS) alone. The aim of this study was to evaluate the impact of several machine perfusion variables (oxygen, temperature as well as timing to start perfusion) on early graft function in a porcine auto-transplant model.
Materials and Methods: The left kidney of a ±40 kg female Landrace pig was exposed to 30 minutes of warm ischemia by vascular clamping and randomized after standard procurement and ex vivo donor blood flush out to one of 6 studied preservation strategies: 1) 22hrs SCS, 2) 22hrs HMP, 3) 22hrs oxygenated HMP, 4) 20hrs HMP + 2hrs NP, 5) 20hrs SCS + 2hrs oxygenated HMP, and 6) 20hrs SCS + 2hrs NP. The LifePort Kidney Transporter® (Organ Recovery Systems) was used for all machine perfusion strategies. The left kidney was auto-transplanted in a right orthotopic position. The primary and secondary endpoints were kidney function and physical parameters during machine perfusion, respectively.
Results:Thirty-seven auto-transplants were performed with a minimum of 6 pigs per study group. Serum creatinine at day 3 after transplantation was significantly lower both in the 22hrs oxygenated (p=0.0011) and non-oxygenated HMP (p=0.0116) group compared to 22hrs of SCS but no treatment effect could be demonstrated between these 2 HMP groups (p=0.3622) at day 3 (figure 1).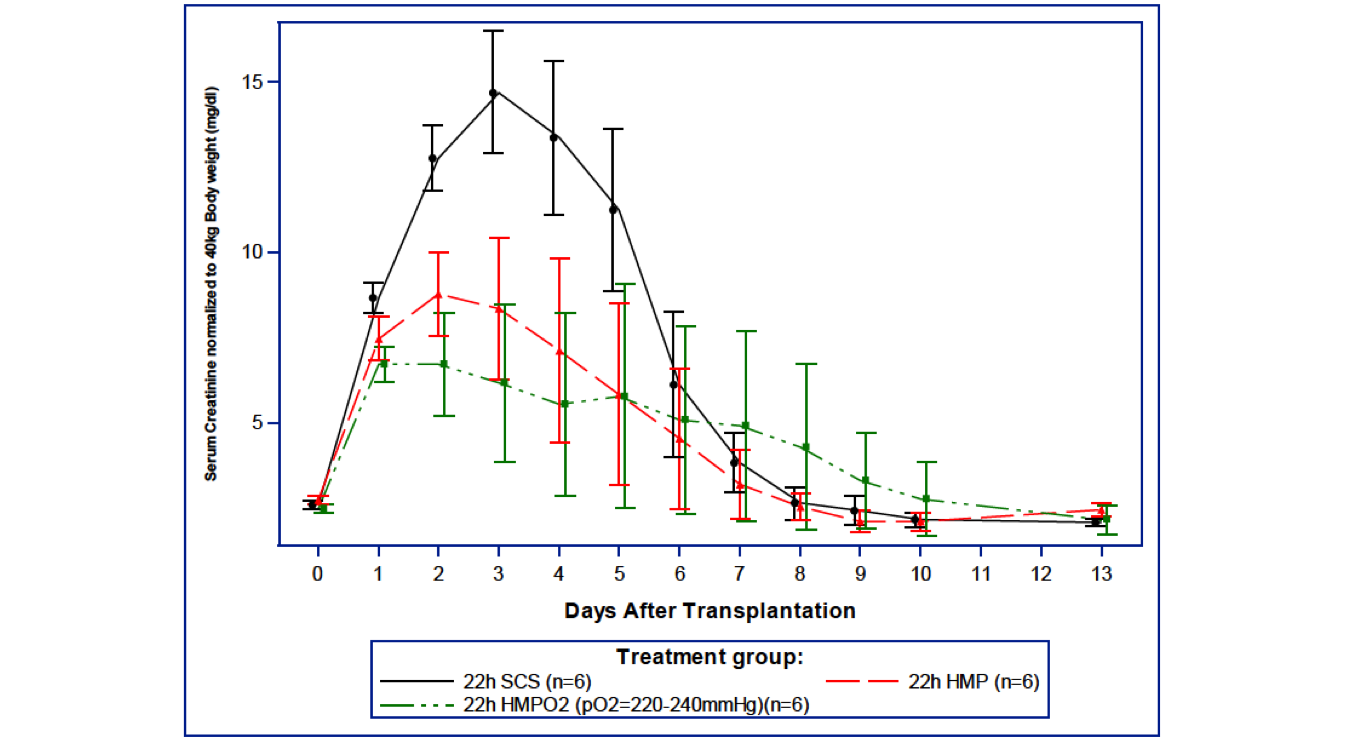 End ischemic strategies could not be demonstrated a statistical significant treatment benefice on early graft function compared to SCS (figure 2).
End ischemic strategies could not be demonstrated a statistical significant treatment benefice on early graft function compared to SCS (figure 2).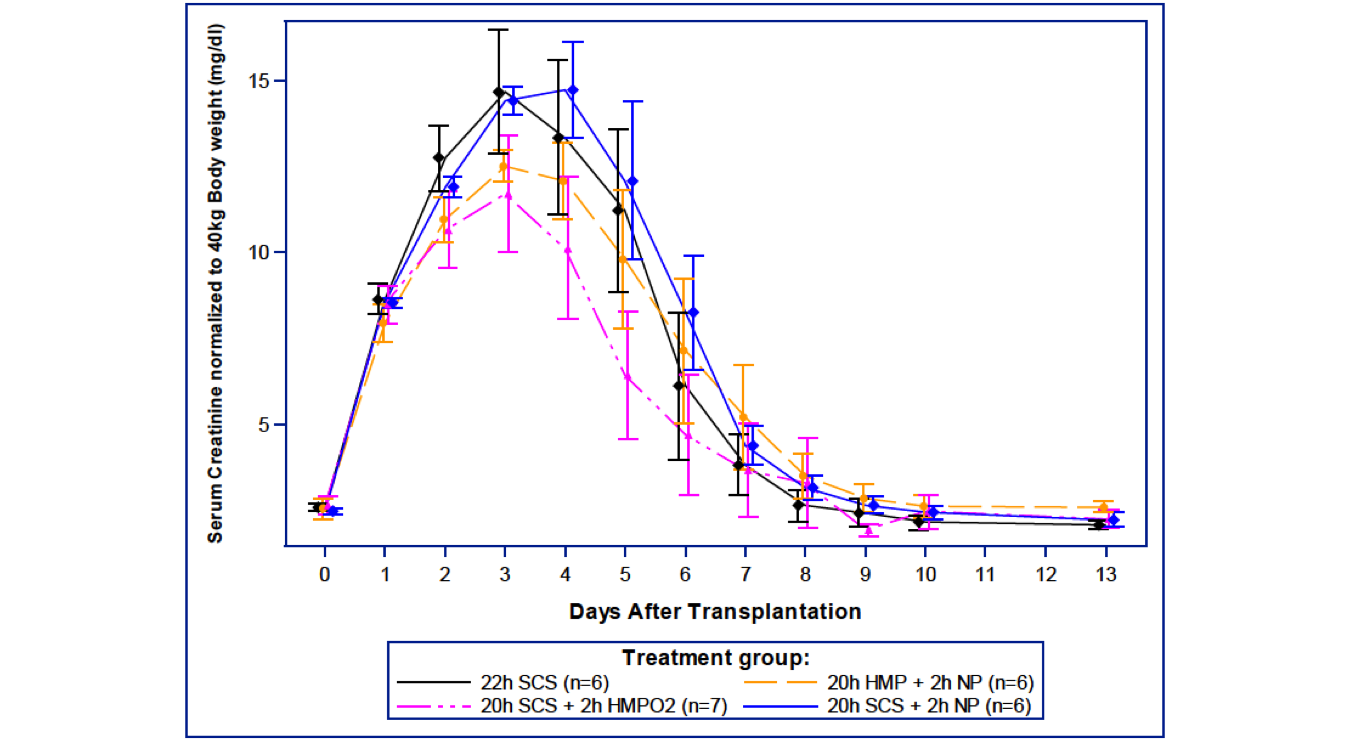 From 8 to 19 hours on machine perfusion the renal blood flow (RBF) was significantly higher in the continuous oxygenated compared to the non-oxygenated HMP group. However RBF at the end of machine perfusion was comparable between these 2 groups (figure 3)(p=0.0812).
From 8 to 19 hours on machine perfusion the renal blood flow (RBF) was significantly higher in the continuous oxygenated compared to the non-oxygenated HMP group. However RBF at the end of machine perfusion was comparable between these 2 groups (figure 3)(p=0.0812).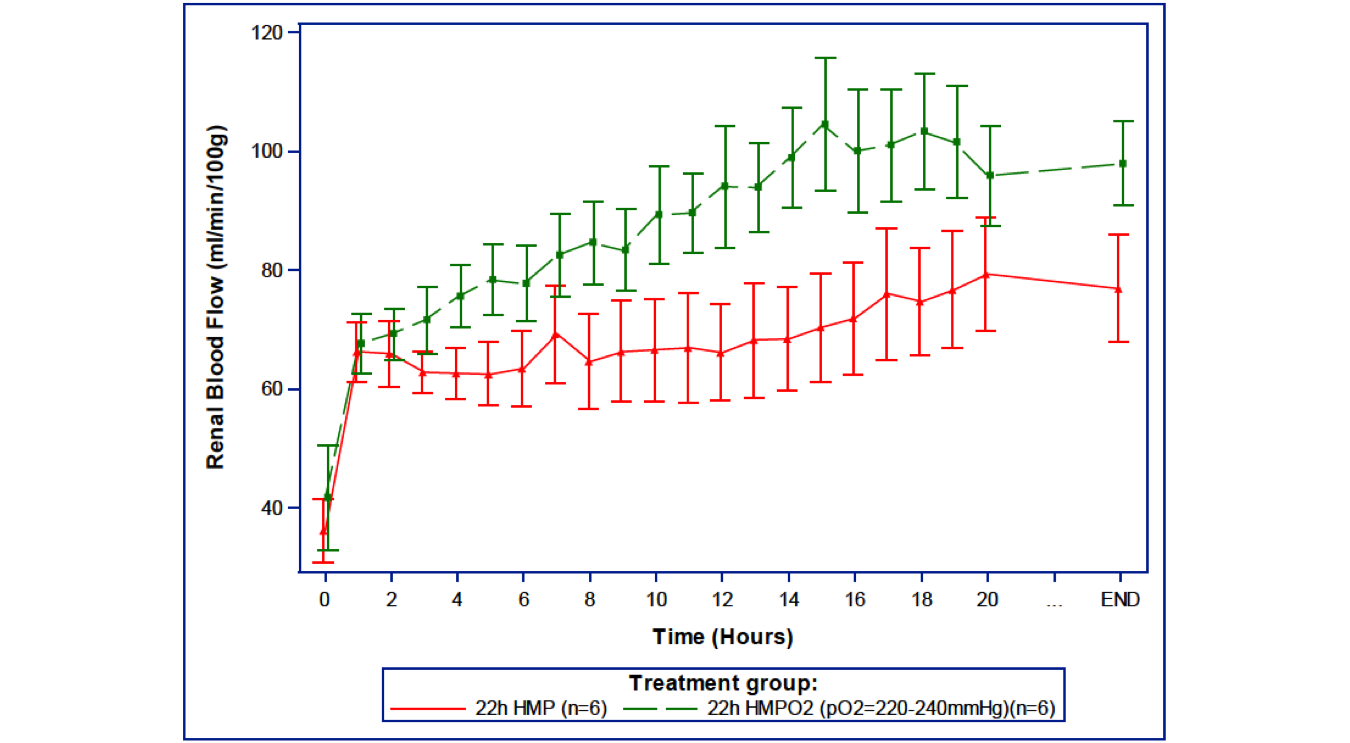 NP results in the highest RBF when performed after HMP (p<0.0001) but no difference in RBF was observed between oxygenated HMPO2/NP after SCS (p=0.31)(figure 4).
NP results in the highest RBF when performed after HMP (p<0.0001) but no difference in RBF was observed between oxygenated HMPO2/NP after SCS (p=0.31)(figure 4).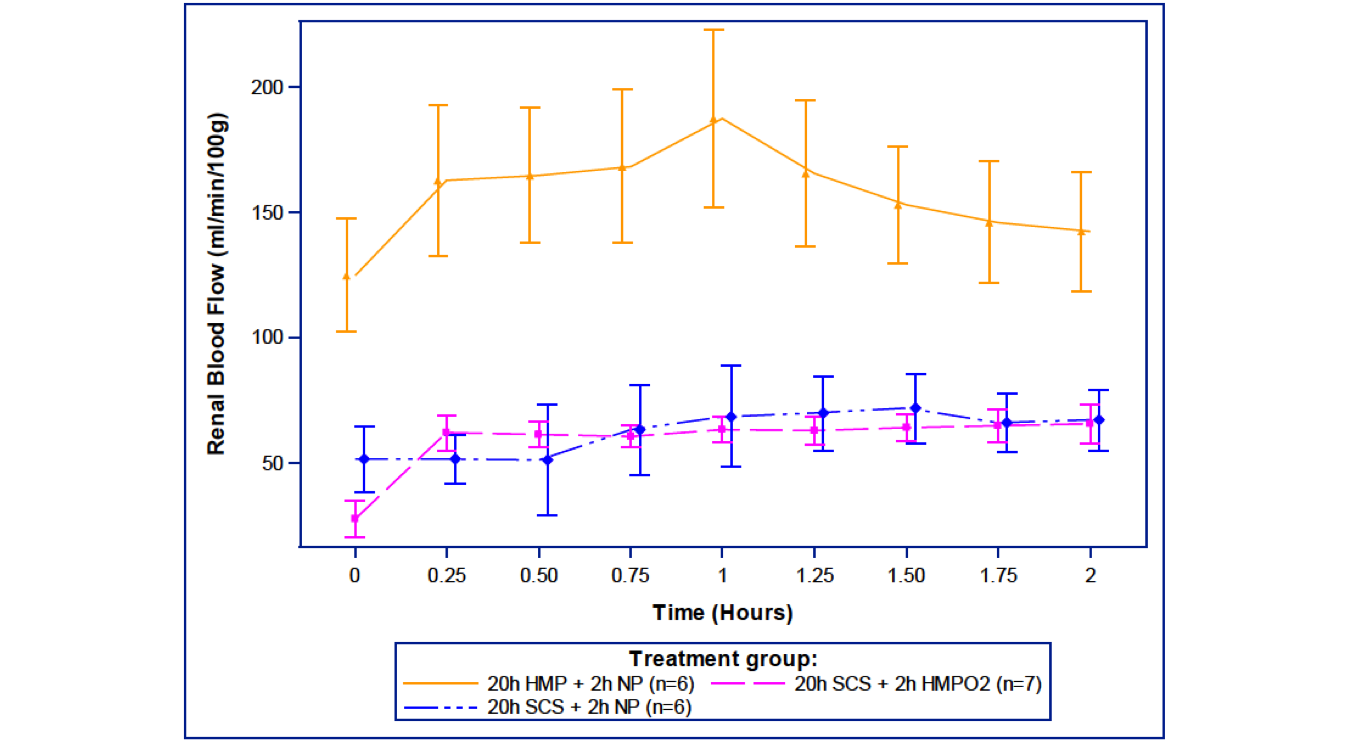
Discussion: Graft recovery from ischemia reperfusion injury was significantly better using continuous HMP strategies compared to end ischemic machine perfusion strategies. Continuous oxygenated HMP demonstrated a faster increase of ex vivo RBF compared to non-oxygenated HMP and better initial graft function, especially during the first week after transplantation.
Conclusions: In this study, hypothermic perfusion strategies only when applied from time of kidney procurement until transplantation and irrespective of supplemental oxygenation, led to a positive effect on early graft function. Continuous oxygenated HMP preservation demonstrated a faster increase of RBF compared to non-oxygenated HMP but without any effect on graft recovery. Further studies are needed to evaluate the effect of oxygen pressure during HMP.
Organ Recovery Systems. Astellas.

