
Comparison of Induction and Maintenance Immunosuppression Regimens in Intestinal and Multivisceral Transplant: An Analysis of the UNOS Registry
Shunji Nagai1, Yakir Muszkat2, Syed-Mohammed Jafri2, Mohamed Safwan1, Randolph Schilke1, Kelly Collins1, Atsushi Yoshida1, Marwan Abouljoud1, Nimisha Sulejmani3, Michael Rizzari1.
1Transplant and Hepatobiliary Surgery, Henry Ford Hospital, Detroit, MI, United States; 2Gastroenterology, Henry Ford Hospital, Detroit, MI, United States; 3Pharmacy, Henry Ford Hospital, Detroit, MI, United States
Aim: Induction and maintenance immunosuppression regimens in intestinal transplant widely vary among centers. The aim of this study was to investigate an association between immunosuppression regimens and transplant outcomes.
Methods: We examined the patients who underwent primary intestinal/multivisceral transplant between January 1, 2001 and March 31, 2017 by using the United Network Organ Sharing registry. Intestine transplant without liver graft group and intestine and liver transplant group were separately analyzed. Patients were categorized based on immunosuppression regimens. Induction regimen groups included none, anti-thymocyte globulin (ATG) with or without rituximab, basiliximab, and alemtuzumab. Additional maintenance agent groups included none, mycophenolic acid, and sirolimus/everlolimus (mTOR-i). Graft and patient survival, death associated with infection, and incidence of acute rejection were evaluated using Cox and logistic multivariable analyses. Risks were adjusted for recipient age/ethnicity/functional status, donor age, and ischemia time.
Results: A total of 1676 patients were eligible for this study (intestine without liver [n=780], intestine with liver [n=896]). In the intestine without liver group, alemtuzumab (hazard ratio [HR]=0.56, P=0.012) and mTOR-i (HR=0.62, P=0.026) showed significantly better graft survival, compared with ATG+rituximab and no additional maintenance agent, respectively. In the intestine with liver group, there was no induction regimen superior to others regarding graft/patient survival, whereas a risk of death associated with infection was lowest in the ATG+rituximab group and highest in the alemtuzumab group (HR=3.324, P=0.034). The mTOR-i group showed significantly better graft outcome in intestine and liver transplant (HR=0.476, P=0.003 [Ref. no additional maintenance agent]).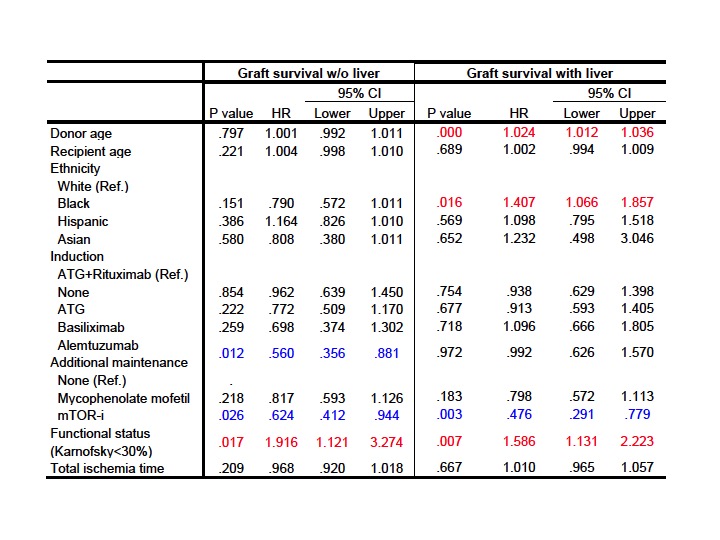 A risk of acute rejection was significantly higher in the groups of ATG alone or almtuzumab, compared with the ATG+rituximab group, regardless of a graft type.
A risk of acute rejection was significantly higher in the groups of ATG alone or almtuzumab, compared with the ATG+rituximab group, regardless of a graft type.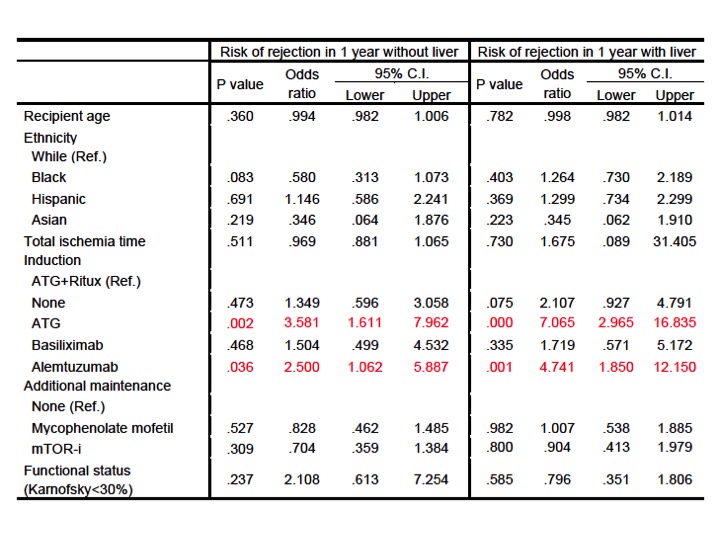
Conclusion: Our results suggested that alemtuzumab induction with mTOR-i as an additional maintenance agent seemed appropriate in intestinal transplant without liver graft, and that ATG+rituximab induction with mTOR-i may be better option in intestinal transplant with liver graft.

