
A New Technique for Cannulation and External ‘Clamping’ in the Difficult DCD Donor
Joshua Hollingshead1, Harvey Solomon MD2,3.
1University of Missouri-Columbia School of Medicine, Columbia, MO, United States; 2Department of Surgery, Saint Louis University School of Medicine, Saint Louis, MO, United States; 3Mid-America Transplant, Saint Louis, MO, United States
Introduction: Donation after Cardiac Death (DCD) in morbidly obese donors, donors with previous abdominal surgeries, pelvic masses, and aortic occlusive or aneurysmal disease present unique challenges for the surgical recovery team. These include increased time required to cannulate after declaration, and increased risk of surgical damage. We propose a new technique to rapidly obtain vascular control and in situ organ flushing in these difficult cases, and our experience with this technique.
Material and Methods: The donor was a 48-year-old, African-American, female, with a BMI of 42.7. After declaration of death, the donor was rapidly prepped and draped in standard fashion. Additionally, the anterior and medial sides of both thighs were prepped and draped. The donor was secured to the table and positioned in a right-side down, reverse Trendelenburg position.
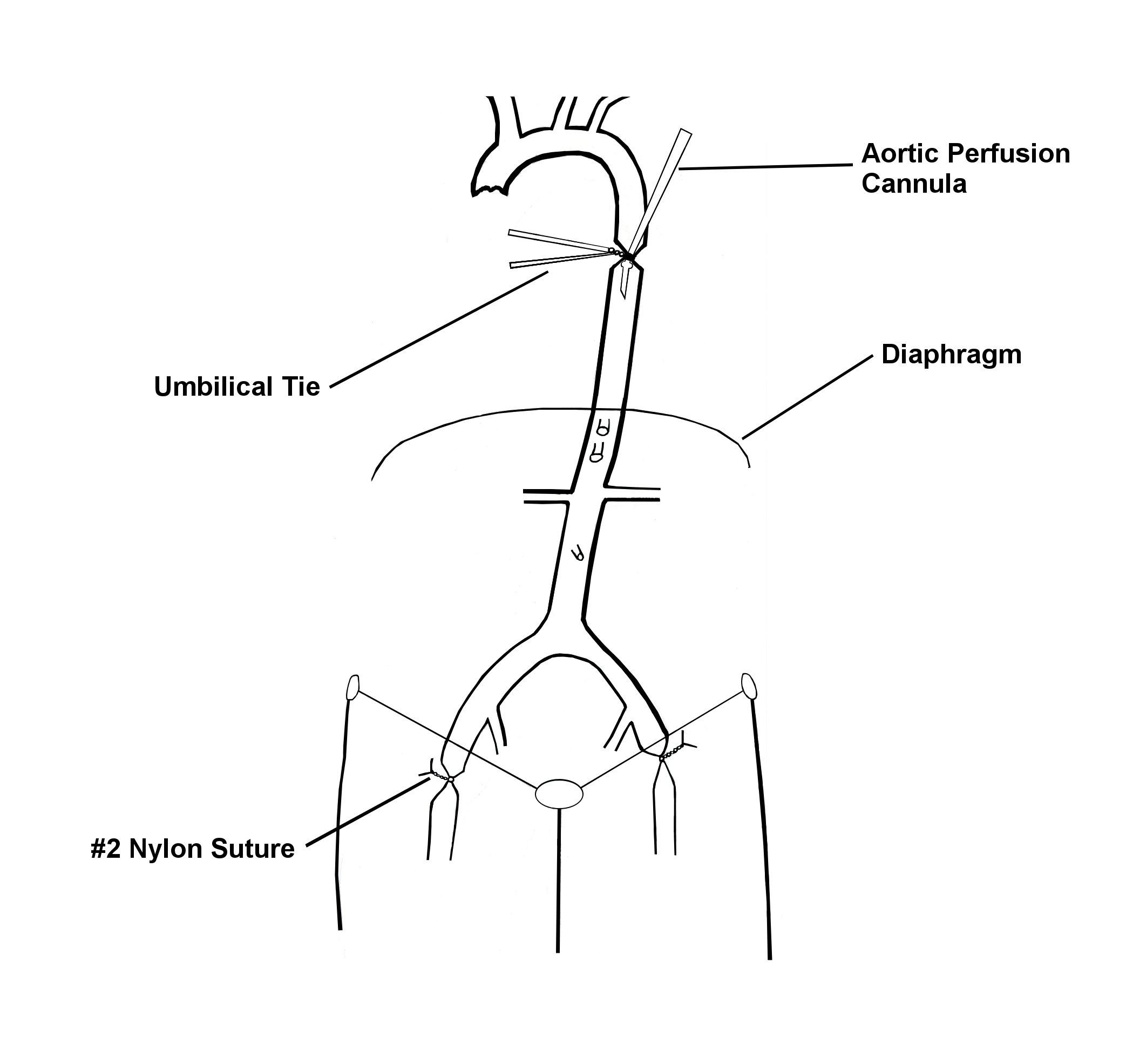
A midline sternotomy was rapidly performed, and the left lung was mobilized to the right. The descending aorta was dissected free of surrounding tissue and encircled with umbilical tape. The mid-descending aorta was incised and a 20 French aortic cannula was placed in the anterograde direction. The cannula was secured with the umbilical tie and the proximal aorta was clamped. The pericardium was opened, a clamp was placed proximally at the IVC-atrial junction, and incised distally for venting purposes. Ice slush was packed into the left and right pleural spaces as inferiorly as possible, in the posterior costophrenic recess, to initiate topical cooling of the kidneys.
While the chest was being opened, a #2 nylon suture on a 75mm 3/8c reverse cutting needle, was inserted deep in each thigh, at the mid-inguinal point, and tied to occlude the femoral vessels. After starting perfusion, a midline laparotomy was performed, and ice was placed on the surfaces of the kidneys. After flushing with 5050 cc of Histidine-Tryptophane-Ketogluterate (HTK), the bilateral donor nephrectomy was continued in standard fashion.
Results and Discussion; In this case, the time to perfusion was less than 3 minutes and flush was rapidly completed. Visually, the kidneys appeared to be sufficiently flushed with preservation solution. Both kidneys experienced delayed graft function, but ultimately achieved excellent function.
Conclusion: We have demonstrated that cannulation of the mid-aorta, and occlusion of the femoral vessels by mass suture can be accomplished rapidly, and is an alternative to clamping the aorta. This technique could be particularly useful as a means of quick cannulation and clamping in DCD donors who are morbidly obese. In addition to this type of donor, it could also be extended to those with aortic aneurysmal disease, a low-lying kidney, renal arteries originating from the iliac arteries, or if the donor has had previous abdominal surgeries. This technique is simple and has the potential to decrease critical time to cannulation, reduce surgical damage, and increase organ yield from DCD donors.

