
Successful Deceased Donor Kidney Transplantation of Highly Sensitized Candidates Across Positive Cross Match and Strong Donor-Specific HLA-DP Antibodies without Desensitization
Raja Rajalingam1, David D Gae1, Zoltan G Laszik2, Mehdi M Tavakol3, Allison B Webber4, Deján Dobi2, Kelly Cunniffe1, Gilberto da Gente1, Ryutaro Hirose3, Garrett Roll3, John P Roberts3.
1Immunogenetics and Transplantation Laboratory, Department of Surgery, University of California, San Francisco, CA, United States; 2Department of Pathology, University of California, San Francisco, CA, United States; 3Transplant Services, Department of Surgery, University of California, San Francisco, CA, United States; 4Division of Nephrology, Department of Medicine, University of California, San Francisco, CA, United States
Introduction: Over 50% of kidney transplant (KTx) candidates with 100% CPRA display HLA-DP antibodies, which impair the chances of finding a compatible deceased donor (DD) despite national sharing. Since the clinical relevance of DP donor-specific antibodies (DSA) is unclear, we do not list DP as unacceptable antigens in UNet. This allowed one of our highly sensitized re-list candidates (99% CPRA + many strong DP antibodies) to receive a kidney offer from a DD that was matched for all HLA loci (16/18 matched) except a single DP1 mismatch. The prospective B cell flow pronase-crossmatch (FXM) was positive (MCS=125; cutoff is 120) due to strong DP1 DSA (MFI=10,930). As the donor was almost HLA-identical and the crossmatch was only borderline positive, we proceeded with this transplantation following anti-CD25 mAb induction. Only a single dose IVIG (2g/kg) at day 1 post-tx was given to block DP1 DSA. The graft was functioning well and rejection was not noted at the 6 month protocol biopsy. Based on this experience, we started to perform KTx across DP DSAs with +/-ve B cell FXM. The aim of the present study was to determine the impact of DP-DSAs on KTx outcome.
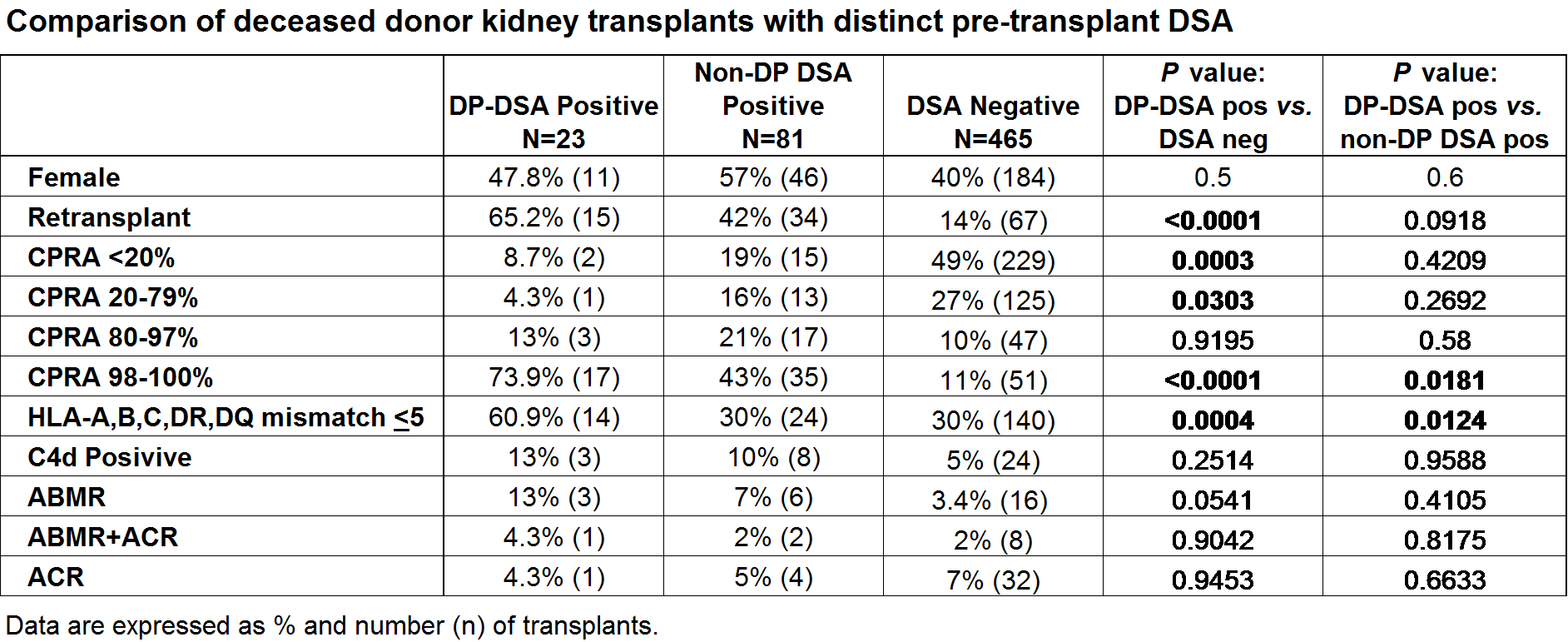
Methods: DD kidney transplants performed from Jan 2013 to Dec 2016 at UCSF were included in this analysis (n=569), divided into 3 groups based on pre-tx DSAs: DSA-negative (n=465), non-DP DSA-positive (n=81), and DP-DSA positive (n=23). Six months protocol biopsies were evaluated for C4d positivity and rejection. One Lambda single antigen bead assay was used for HLA antibody testing.
Results: The number of very highly sensitized patients (98-100% CPRA) and well-matched transplants (<5 out of 10 HLA-mismatches) were significantly higher in DP-DSA positive group compared to other two transplant groups (Table). None of the recipients in DSA-negative or in non-DP DSA positive groups had a positive flow XM, while 30.4% (n=7) in DP-DSA positive group that had a DP-DSA of >10,000 MFI were positive by B cell flow XM (~200 MCS). There were no hyper acute rejection episodes in all 3 groups. The levels of DP-DSAs decreased overtime following KTx in all 23 recipients (Figure). The 6-month protocol biopsy findings revealed no significant difference in the rate of antibody-mediated rejection (ABMR) or in acute cellular rejection (ACR) between the 3 groups. Two recipients with DP-DSAs lost their grafts: one was a 46F re-tx recipient with 100% CPRA, 1/12 HLA-mismatch, DP4 DSA (MFI=6956), lost due to ACR in 4 months; another was 62M, 19% CPRA, 7/12 HLA-mismatch, DP1 DSA (MFI=4165) suffered Polymavirus nephropathy at 5 months.
Conclusions: Patients can be transplanted across HLA-DP DSAs with no readily apparent effect on graft survival. Given the prevalence of DP antibodies in highly sensitized candidates, this strategy significantly increases the likelihood of highly sensitized candidates receiving compatible DD offers. Studies assessing the long-term outcome in these recipients are ongoing.

