
The Impact of Age-Matching on Graft Function and Graft Survival After Living Donor Kidney Transplantation
Jee Youn Lee1, Deok Gie Kim1, Jae Geun Lee1, Juhan Lee1, Yoon Bin Jung1, Soo Jin Kim1, Man Ki Ju1, Sung Hoon Kim2, Kyu Ha Huh1, Beom Seok Kim3, Soon Il Kim1, Yu Seun Kim1, Myoung Soo Kim1.
1Department of Surgery, Yonsei University College of Medicine, Seoul, Korea; 2Department of Surgery, Yonsei University Wonju College of Medicine, Wonju, Korea; 3Department of Internal medicine, Yonsei University College of Medicine, Seoul, Korea
Introduction: The number of patients on the waiting list for kidney transplants is increasing. To overcome the shortage of organs, the influence of age matching in deceased donor kidney transplantation(DDKT) has been studied, but there is no enough data for living donor kidney transplantation (LDKT). We analyzed the impact of age-matching on graft function and graft survival after LDKT.
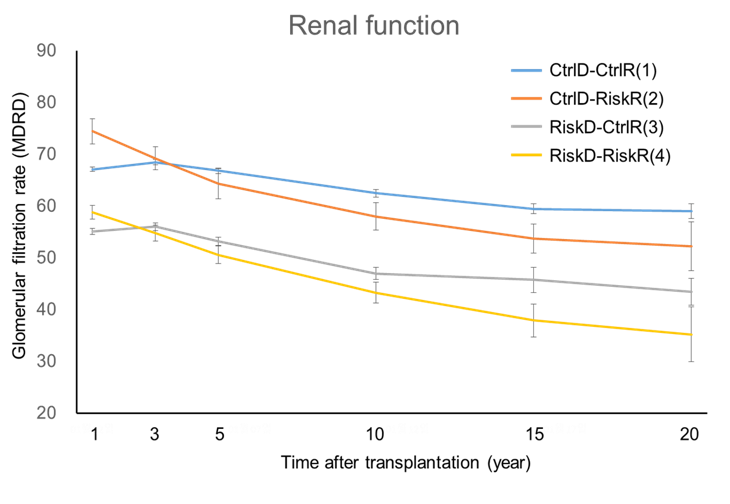
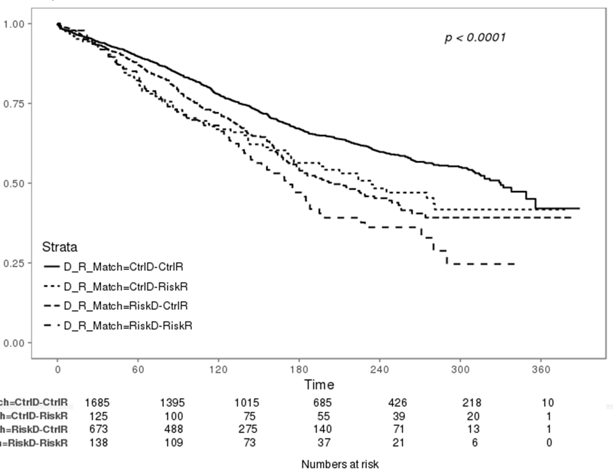
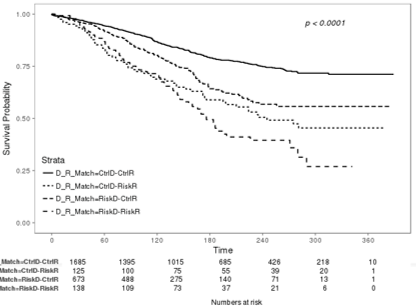
Method: The data of 2621 recipients who underwent LDKT were reviewed. Patients were divided into four groups according to the cutoff values of donor age 45 years and recipient age 25 years; CtrlD-CtrlR, CtrlD-RiskR, RiskD-CtrlR, and RiskD-RiskR. The renal function, the total graft survival and the death censored graft survival were compared among the groups.
Result: At 1, 3, 5, 15, and 20 years after transplant, the estimated glomerular filtration rate(eGFR) of recipients from control donor was significantly higher than that of recipients from risk donor regardless of recipient age group (Control recipients, P<0.001; Risk recipients, P=0.005). When we compare the total graft survival rate for 20 years, CtrlD-CtrlR showed the highest survival rate and RiskD-RiskR showed the worst survival rate (P<0.001). When we compare death censored graft survival, the result was amplified (P<0.001). In multivariate analysis, pretransplant dialysis, acute rejection within 1year and age group were the independent risk factor for death censored graft survival.
Conclusion: The younger living donors provide the best outcomes for recipients regardless of the age. This should be considered at the time of donor evaluation, especially when several donors are available. For elderly recipients, the next best alternative option is receiving old living kidneys rather than dialysis or DDKT.

