

Cognitive Impairment and Graft Loss in Kidney Transplant Recipients
Alvin Thomas1, Jessica Ruck1, Ashton Shaffer1,3, Christine Haugen1,3, Hao Ying1, Fatima Warsame1, Nadia Chu3, Michelle Carlson3, Alden Gross3, Silas Norman2, Dorry Segev1, Mara McAdams DeMarco1,3.
1Surgery, Johns Hopkins, Baltimore, MD, United States; 2Medicine, University of Michigan, Ann Arbor, MI, United States; 3School of Public Health, Johns Hopkins, Baltimore, MD, United States
Background: Cognitive impairment is common in end-stage renal disease patients and impairs adherence to complex treatment regimens. Given the need for post-transplant immunosuppression, we hypothesized that cognitive impairment at the time of transplant is associated with an increased risk of all-cause graft loss (ACGL) among kidney transplant (KT) recipients.
Method: Using the Modified Mini-Mental State (3MS) examination, we measured global cognitive function in a prospective cohort of 864 KT candidates (8/2009-7/2016) as part of a multi-center, prospective cohort study. We estimated the association between pre-KT cognitive impairment and ACGL using Cox regression adjusting for recipient, donor, and transplant factors. We then estimated the national prevalence of cognitive impairment in US KT recipients using multiple imputation by chained equations and predictive mean matching.
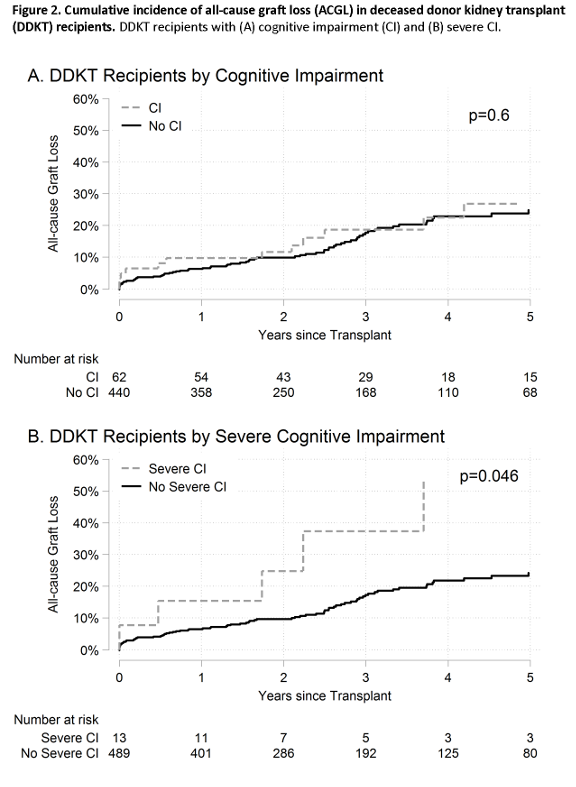
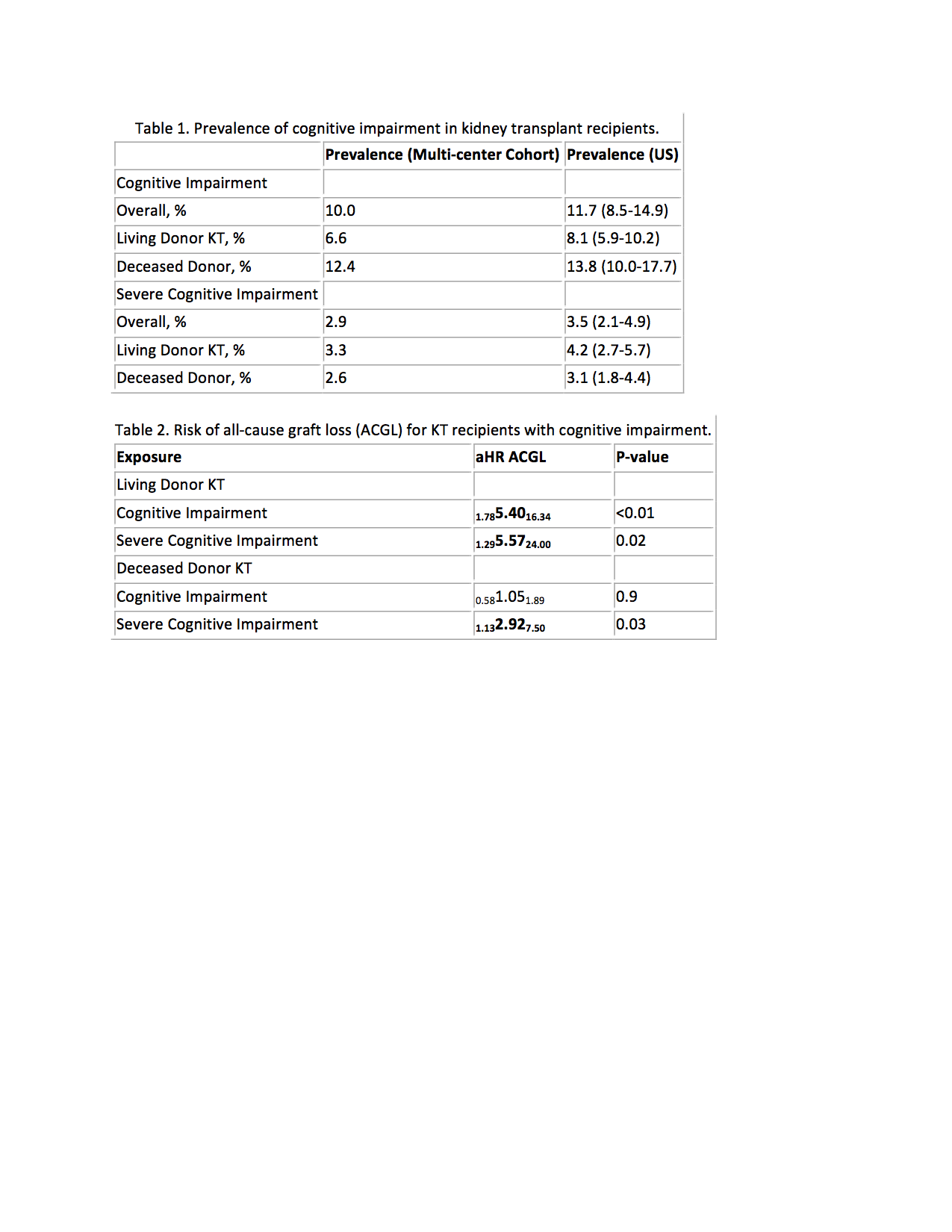
Results: The prevalences of impairment (3MS<80) and severe impairment (3MS<60) were 6.6% and 3.3%, respectively, among living donor KT (LDKT) recipients and 12.4% and 2.6%, respectively, among deceased donor KT (DDKT) recipients. Projected nationally, 11.7% (8.5-14.9%) of all KT recipients had cognitive impairment during the study period (Table 1). LDKT recipients with impairment had higher ACGL risk than recipients without impairment (5-year ACGL: 45.5% vs. 10.6%, p<0.01; aHR impairment: 1.785.4016.34, p<0.01; aHR severe impairment: 1.295.5724.00, p=0.02) (Table 2, Figure 1). DDKT recipients with severe impairment had higher ACGL risk than recipients without severe impairment (5-year ACGL: 53.0% vs. 24.2%, p=0.04; aHR severe impairment: 1.132.927.50, p=0.03) (Figure 2).
Conclusion: Given the prevalence of cognitive impairment and the associated higher ACGL risk, pre-KT screening for impairment is warranted to identify higher-risk KT recipients.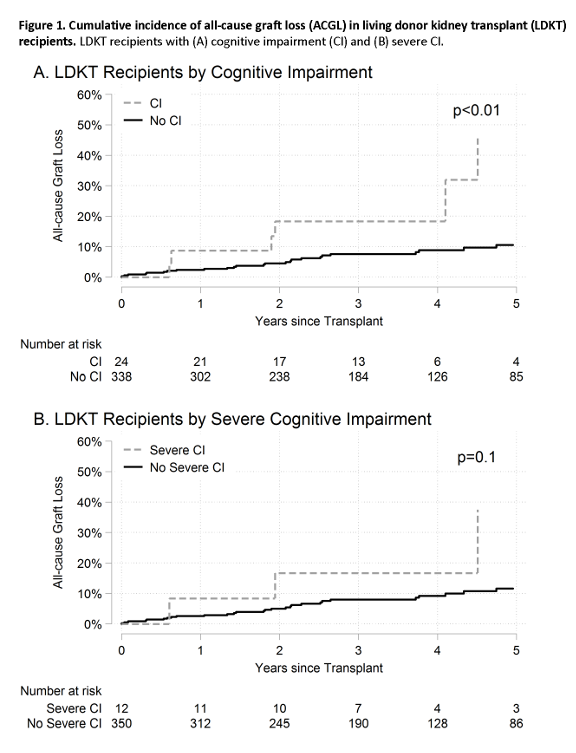
National Institute of Diabetes and Digestive and Kidney Disease (NIDDK) and the National Institute on Aging (NIA); grant numbers K01AG043501 (PI: Mara McAdams-DeMarco), R01AG055781 (PI: Mara McAdams-DeMarco), F30DK116658 (PI: Ashton Shaffer), F32AG053025 (PI: Christine Haugen), K01AG050699 (PI: Alden Gross), K24DK101828 (PI: Dorry Segev), and R01DK096008 (PI: Dorry Segev). Additionally, Jessica Ruck and Dorry Segev are supported by a Doris Duke Charitable Foundation Clinical Research Mentorship grant..

