
Significance of Cytomegalovirus Specific T Lymphocytes in Kidney Transplant Recipients
Maciej Zieliński1, Agnieszka Tarasewicz2, Magdalena Jankowska2, Hanna Zielińska1, Grażyna Moszkowska1, Alicja Dębska-Ślizień2, Bolesław Rutkowski2, Piotr Trzonkowski1.
1Department of Clinical Immunology and Transplantology, Medical University of Gdańsk, Gdańsk, Poland; 2Department of Nephrology, Transplantology and Internal Diseases, Medical University of Gdańsk, Gdańsk, Poland
Introduction: CMV viremia is routinely used to confirmed CMV infection after kidney transplantation. Also, immune assays can be applied to predict viremia development or guiding prophylaxis and preemptive therapies. Most of the immunological assays rely on functional methods that detect INFγ after stimulation of lymphocytes with viral peptides. There is also MHC multimers assay that identifies antigen-specific lymphocytes crucial for controlling virus latency. It was proved for allogeneic stem cell transplant recipients that levels 2 to 10 cells/µl can successfully protect against CMV infection. Unfortunately, it is not for kidney transplant recipients. We hypothesize that CD28 expression may serve as an additional functional marker for viral-specific lymphocytes, as CD28 occurs with CMV infection and it is linked with early, intermediate and late antigen-specific T lymphocytes differentiation status. Thus, the aim of these study was to verify whether the CMV specific T lymphocytes or extended phenotype of CMV specific T lymphocytes may be used as a marker of CMV viremia in kidney transplant recipients.
Materials and Methods: CMV viremia was monitored in 52 kidney transplant recipients every three months, in two-years lasting follow-up. CMV specific lymphocytes were measured as CD8+ lymphocytes using MHC multimer assay. Further, CMV specific lymphocytes were assessed for CD28 expression (Figure 1).
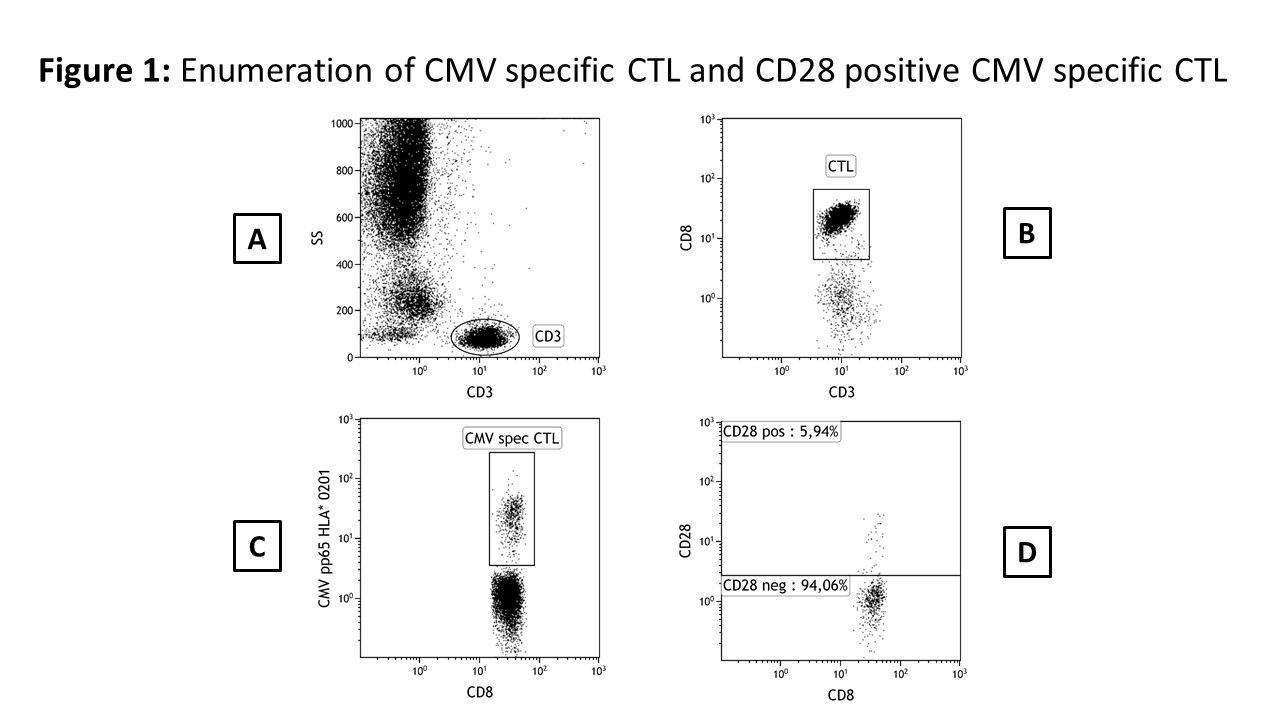
Values were reported both as percentages as well as absolute cell count.
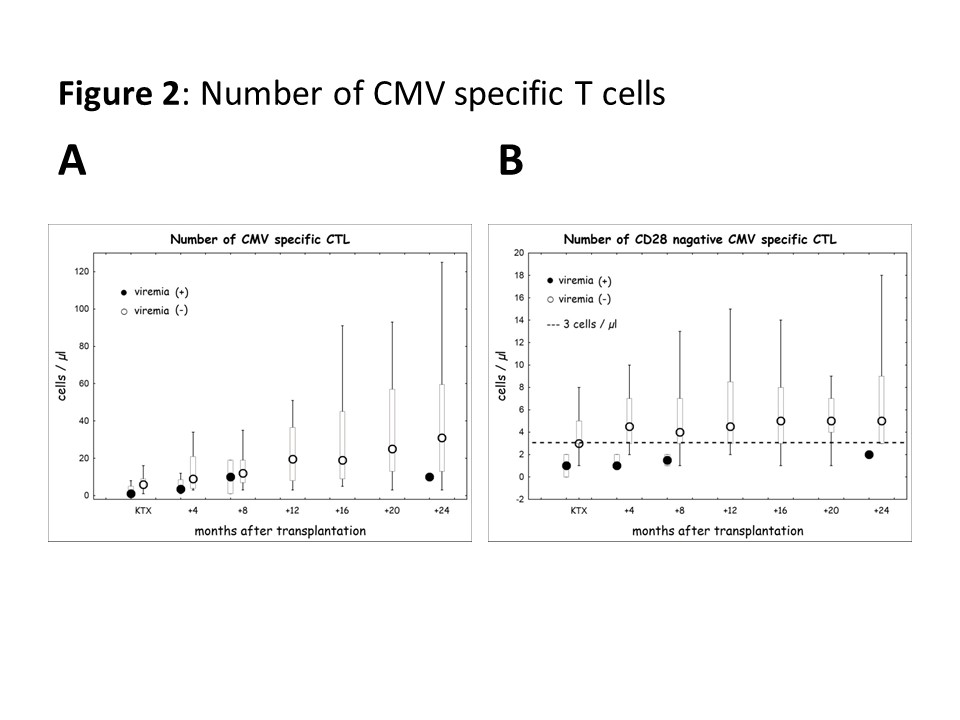
Results and Discussion: CMV specific CD8+ T cells, expressing CD28 were superior for identification of patients at risk of viremia development after kidney transplantation. A cut-off value below 3 cells/µl successfully predict CMV viremia with acceptable specificity and sensitivity confirmed by ROC analysis, AUC values 0,774 – 0,951 depends on time posttransplant (Figure 2).
The overall risk of CMV viremia was strongly associated with donor/recipient (D/R) serological status before transplantation, analyzed with Kaplan-Meier survival analysis (Figure 3).
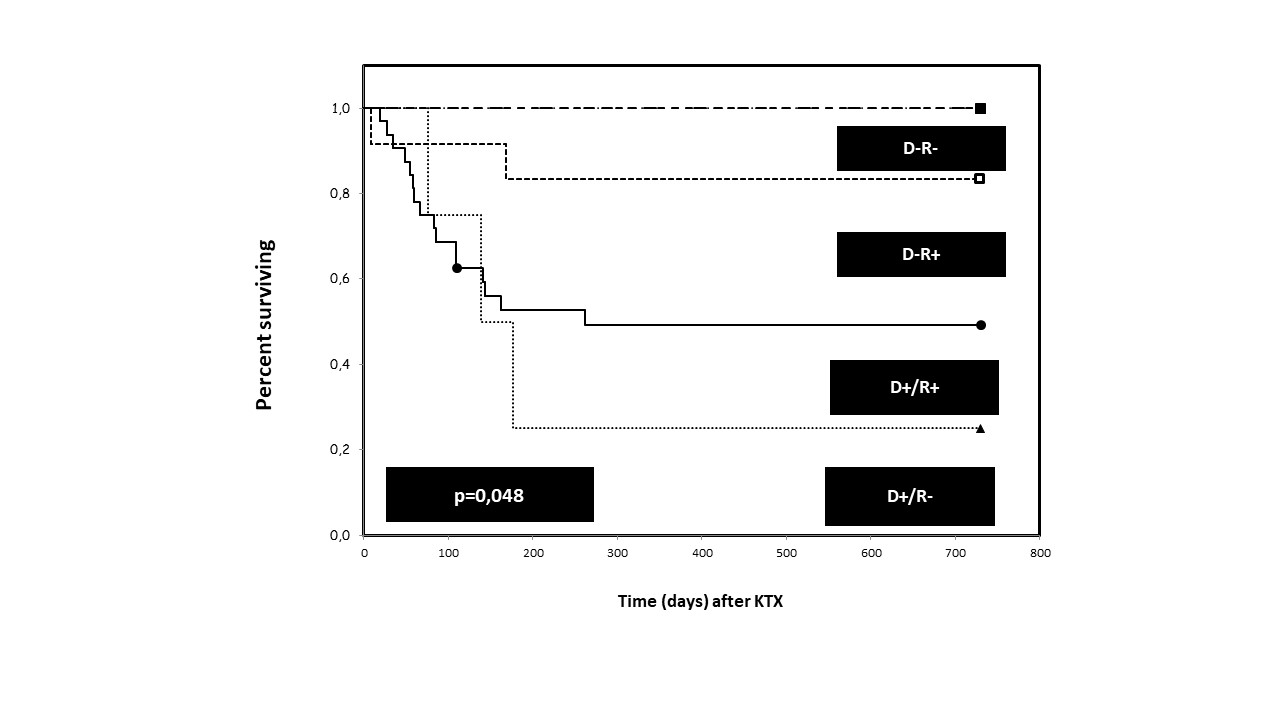
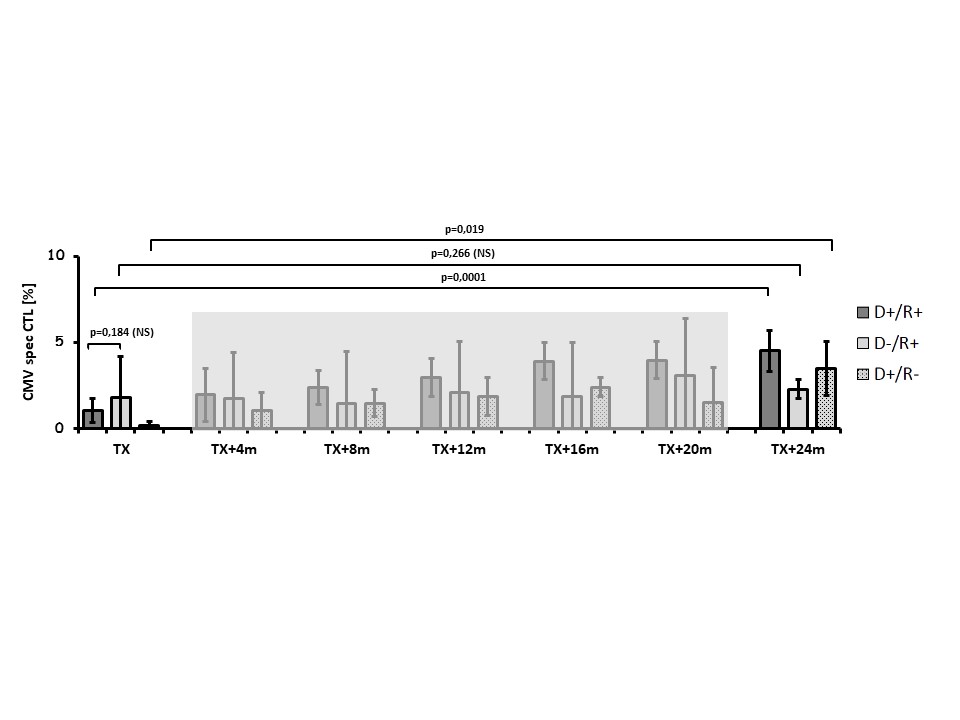
The highest risk of viremia development was associated with CMV primary infection (D+/R-). Interestingly, CMV positive recipients transplanted from CMV positive donor (D+/R+) had a higher risk of viremia when compared to uninfected donors (D-/R+), despite increased levels of CMV specific T lymphocytes (Figure 4).
Conclusion: Collectively, CMV specific T lymphocytes testing enables personalized assessment of recipient’s immune system. This data may be used for CMV viremia risk stratification, that could be applied for tailored pharmacotherapy after kidney transplantation.
National Centre for Research and Development, Poland (No. STRATEGMED1/233368/1/NCBR/2014). National Science Centre, Poland (No. NN402420738 and NN402562440).

