

Inclusion of Incompatible Directed Deceased Donor Organs in Kidney Transplant Exchanges
Ernesto Molmenti1, Christine L Sardo Molmenti2, Elliot Grodstein1, Horacio Rilo1, Lewis W Teperman1.
1Surgery/Transplant Surgery, Northwell Health, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Manhasset, NY, United States; 2Occupational Medicine, Epidemiology and Prevention, Northwell Health, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Great Neck, NY, United States
In many instances, kidney transplants cannot be performed because of incompatibility (such as blood type or cross-match) among donors and recipients. One established way to address this finding is by means of donor exchanges, where incompatible pairs are enrolled in a registry. Registries can lead to paired exchanges or to donor chains. In chains, a non-directed (altruistic) donor initiates a sequence of transplants that culminates with a so-called bridge-donor. Studies have estimated that a non-directed donor triggers on average 4.8 to 8 (if blood type O) transplants (1).
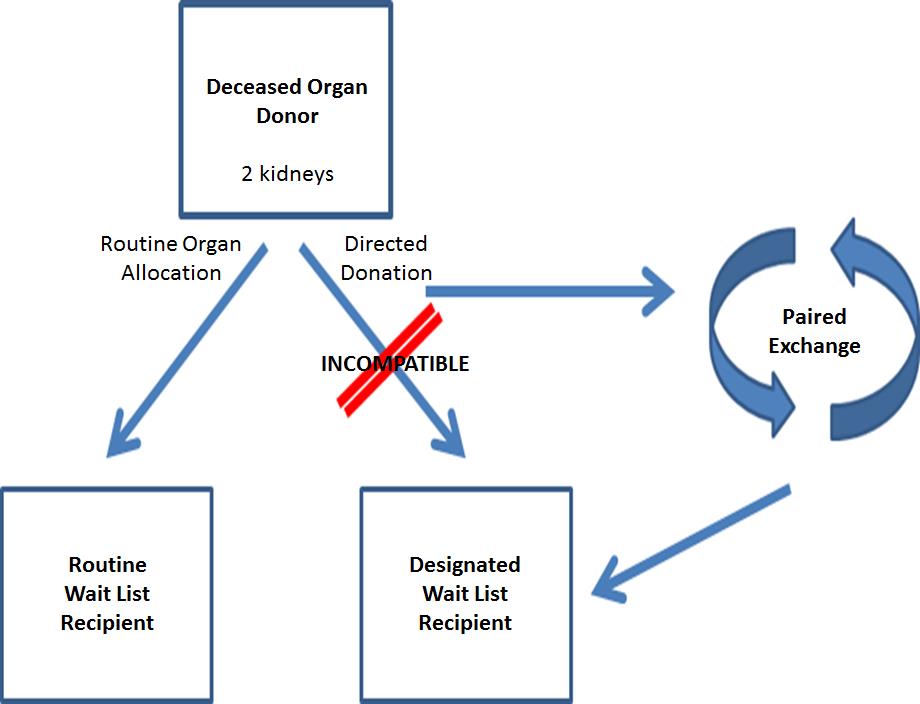
Although incompatibility is usually viewed as affecting potential recipients of live donors, it is also encountered in instances of directed donation of deceased donors. In these cases, the family or guardian of a deceased donor requests that an organ be assigned to a recipient of their choice (such as a relative or friend) in the deceased donor wait list. It has been reported (2) that “in recent years, at least 100 deceased donor transplants each year have occurred through directed donation.”
Although most chains involve only live donors, current proposals (1) consider the initiation of chains with deceased donors. Arguments for such approach include an increased overall number of transplants by maximizing the potential of chains, and the eventual return of a live donor kidney to the deceased donor wait list. Ethical and organizational concerns have been raised with respect to the initiation of chains with deceased donors. Furthermore, selecting blood type O donors to initiate chains could disadvantage blood type O wait list recipients.
We believe it would be particularly interesting to develop exchanges (as diagrammed below) initiated with deceased donor kidneys from incompatible directed donations. Rather than denying the donor family and the designated recipient the possibility of a transplant, the organ would be allocated to initiate an exchange. As part of the exchange, the previously incompatible recipient would receive a compatible live donor kidney.
Advantages of this exchange include:
References:
1- https://optn.transplant.hrsa.gov/media/2219/kidney_pcconcepts_201707.pdf
2- https://optn.transplant.hrsa.gov/news/optn-information-regarding-deceased-directed-donation/

