
Impact of Machine Perfusion on Delayed Graft Function and Graft Survival from High-Risk Donors
Larissa Andrade1,2, Frederico Cavalcanti1,2, Lucila Valente1,2.
1Nefrologia, Real Hospital Português de Beneficência de Pernambuco, Recife, Brazil; 2Nefrologia, Hospital das Clínicas da Universidade Federal de Pernambuco, Recife, Brazil
Introdution: Kidney transplantation (KT) is the treatment of choice for patients with end-stage chronic kidney disease. After KT, the graft may not function immediately and the patient needs to undergo dialysis, characterizing delayed graft function (DGF). DGF increases length of hospital stay, costs and reduces graft survival. The incidence of DGF is higher in expanded criteria donor (ECD), prolonged cold ischemia time (CIT) and donors with renal dysfunction. There are two methods of renal preservation: the traditional, cold storage (CS) and machine perfusion (MP). MP is a high-cost technology, restricted to few hospitals and studies showed that it reduces the incidence of DGF.
Objectives: Analyze the incidence of DGF, its duration, CIT, length of hospital stay, graft and patient survival one year after transplantation and renal function estimated by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation at 1, 3, 6, 9 and 12 months in patients transplanted with CS kidneys compared to MP after CS. Methods: This study was retrospective cohort, in a single center. We included transplants from DCE or standard deceased donors if CIT ≥ 24 hours, cardiorespiratory arrest before donation or creatinine ≥1.8mg/dL prior to retrieval from January 2015 to December 2016 with 1 year follow up.
Results: Sample was 92 patients, 52 transplanted with kidneys in MP. Demographic characteristics were similar between groups except for age of recipient that was higher in the MP group, p=0.03 and donor creatinine prior to retrieval which was 0.7mg/dL higher in the CS group, p=0.01. 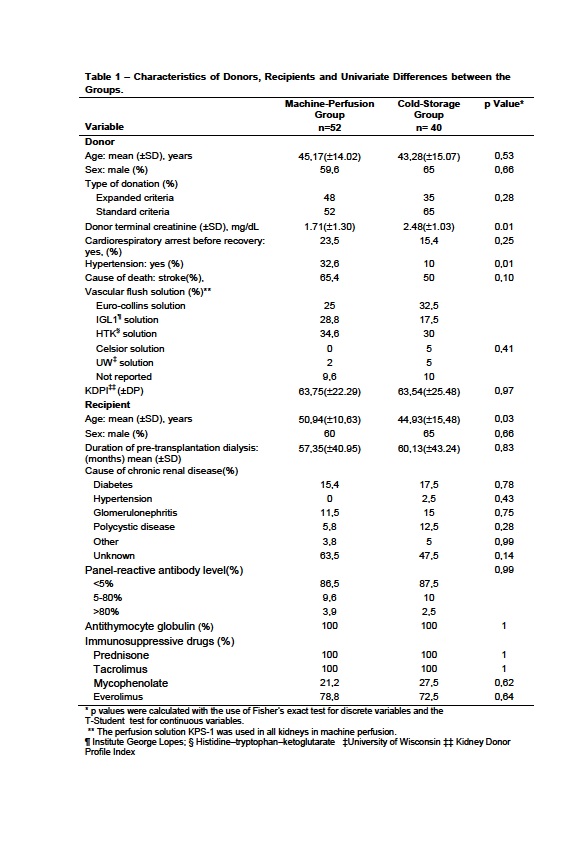 The incidence of DGF was 86.5% in the MP group and 95% in the CS group, p=0.29. There was no difference in DGF duration between groups. The MP patients remained 7 days less hospitalized than the patients in CS, p = 0.15. CIT was 8.19 hours higher in the MP group, p<0.01. CIT of kidneys in MP was 13.63 hours.
The incidence of DGF was 86.5% in the MP group and 95% in the CS group, p=0.29. There was no difference in DGF duration between groups. The MP patients remained 7 days less hospitalized than the patients in CS, p = 0.15. CIT was 8.19 hours higher in the MP group, p<0.01. CIT of kidneys in MP was 13.63 hours. 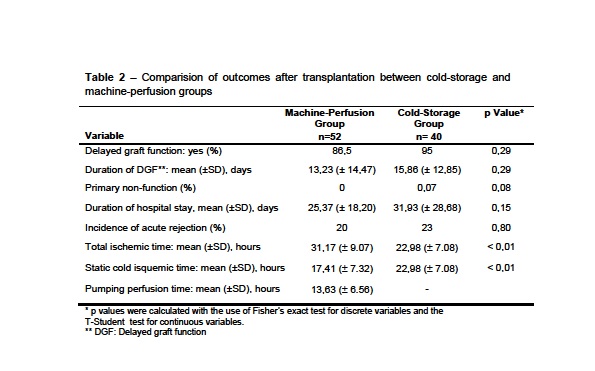 Graft survival was 90.4% in the MP group and 87.5% in the CS patients, p = 0.69.
Graft survival was 90.4% in the MP group and 87.5% in the CS patients, p = 0.69. 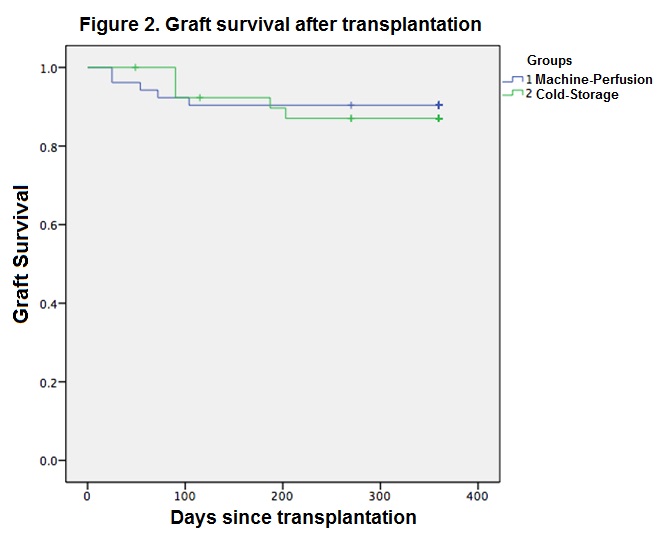 Patient survival was 94.2% in the MP group and 95% in the PE group, p = 0.86. There were no differences in creatinine clearances at 1, 3, 6, 9 and 12 months. One year after transplantation, 89.6% of MP patients and 66.7% of CS group had creatinine clearance higher than 30mL/min/1.73m2, p=0.01.
Patient survival was 94.2% in the MP group and 95% in the PE group, p = 0.86. There were no differences in creatinine clearances at 1, 3, 6, 9 and 12 months. One year after transplantation, 89.6% of MP patients and 66.7% of CS group had creatinine clearance higher than 30mL/min/1.73m2, p=0.01.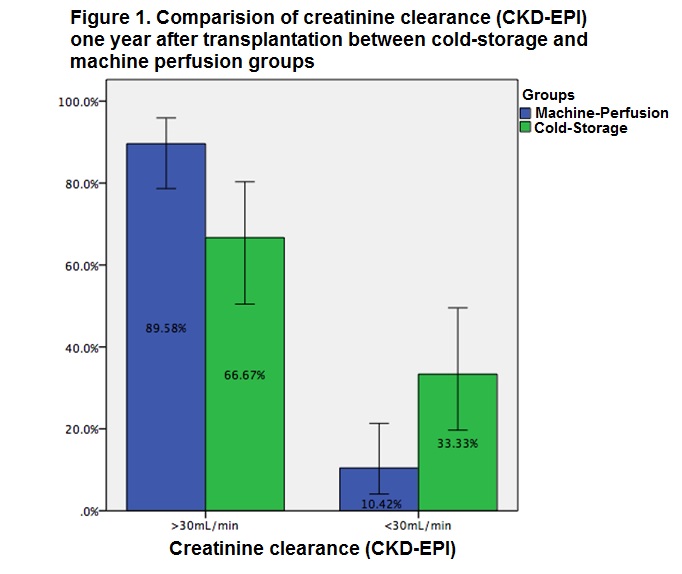 In the multivariate analysis, risk factors for worse graft function at 1 year were: donor age (OR 1.11 CI95% 1.01-1.22; p=0,03) and CS preservation (OR 6.52 CI 95% 1.46-29.08; p=0.01). Conclusions: The incidence of DGF was high and there were no statistical differences between the groups. The higher CIT in the MP group did not increase incidence of DGF. Patients in the MP group were hospitalized 7 days less than the CS group, although there was no statistical difference. Patient and graft survival were high one year after KT, no differences between groups. MP showed better graft function one year after KT.
In the multivariate analysis, risk factors for worse graft function at 1 year were: donor age (OR 1.11 CI95% 1.01-1.22; p=0,03) and CS preservation (OR 6.52 CI 95% 1.46-29.08; p=0.01). Conclusions: The incidence of DGF was high and there were no statistical differences between the groups. The higher CIT in the MP group did not increase incidence of DGF. Patients in the MP group were hospitalized 7 days less than the CS group, although there was no statistical difference. Patient and graft survival were high one year after KT, no differences between groups. MP showed better graft function one year after KT.

