A Case of Urinary Bladder Squamous Cell Carcinoma Post Renal Transplant with a Previous History of Bilharziasis
Ashraf Attia1, Mohamed Saied1, Salem Alqurashi1, Ahmad Chabalout1, Ihab Mahmoud1, Rafat Zahed1, Alawi Altaweel1, Mohamed Elamin1, Nagoud Ali1.
1Nephrology, Prince Sultan Military Medical City, Riyadh, Saudi Arabia
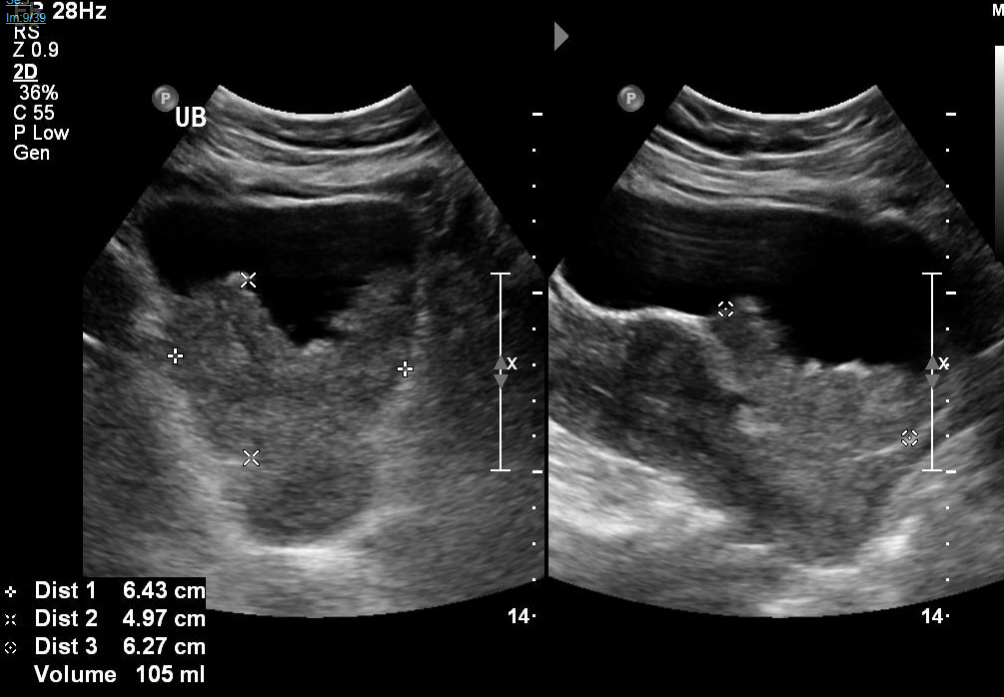
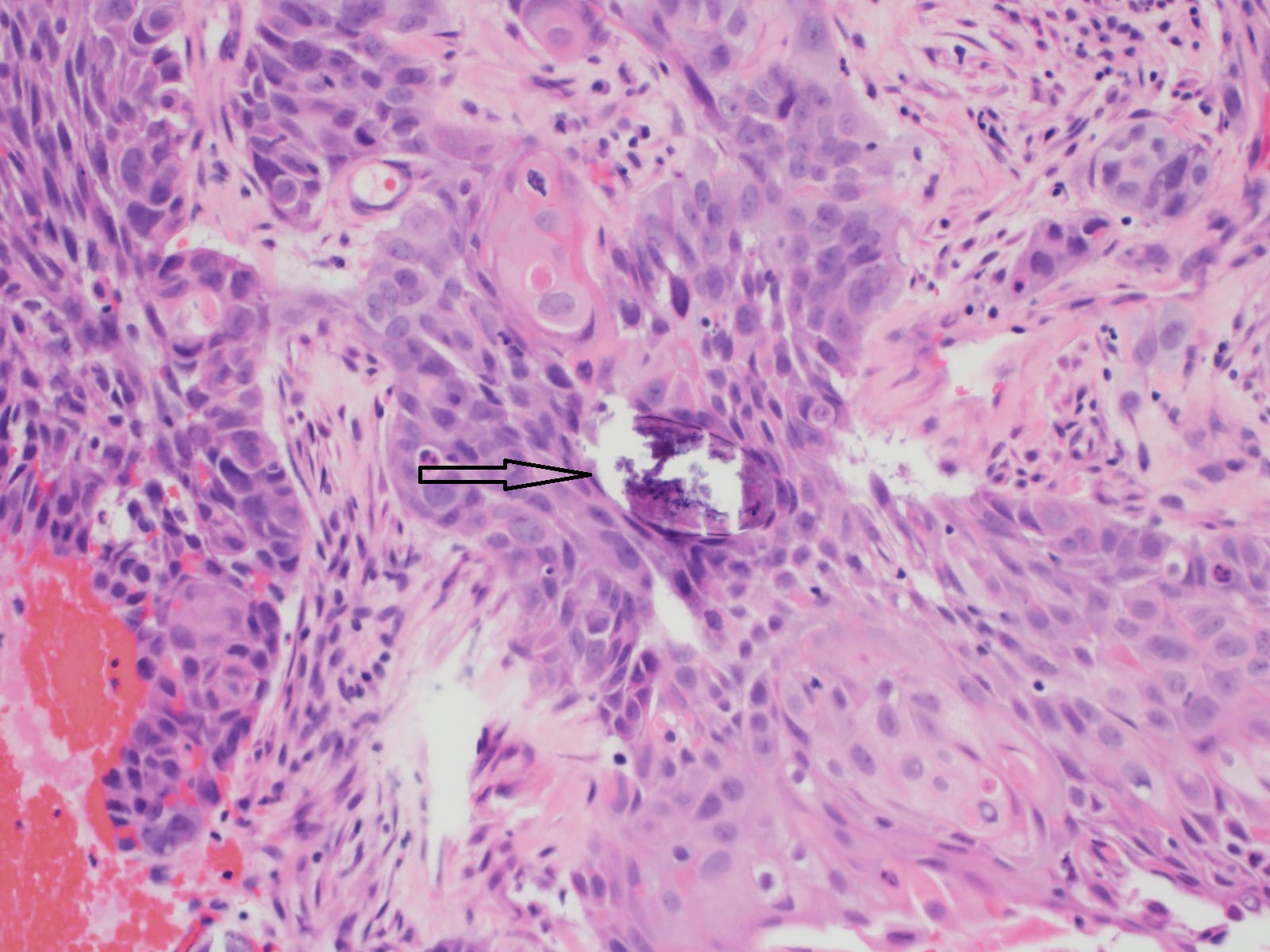
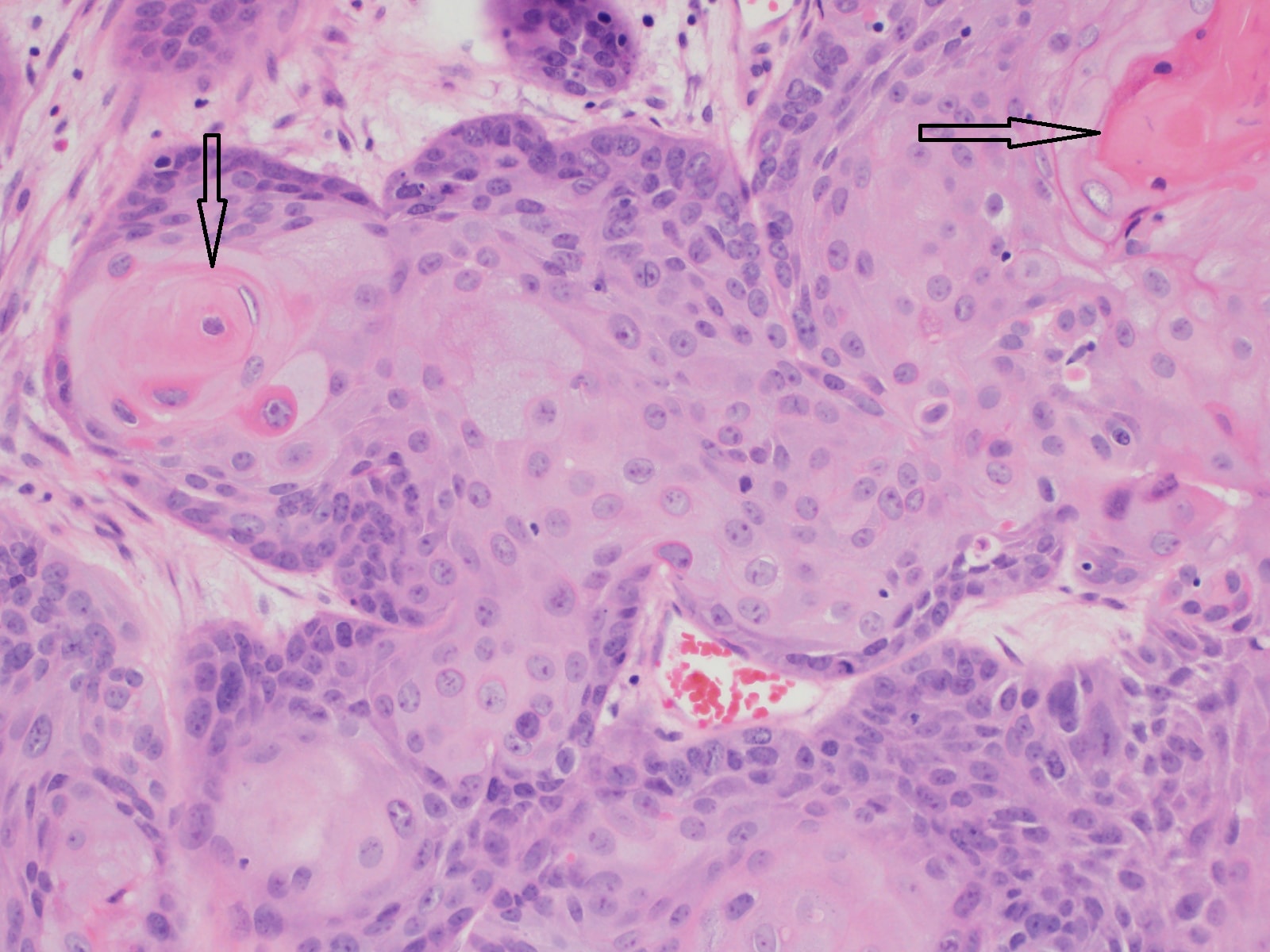
We report a case of post renal transplant urinary bladder squamous cell carcinoma on top of shishtosomiasis, a female patient got living non related renal transplant 2015 her primary investigations showed anti shistisoma titer of 1/80, urine analysis was negative for bilharzial ova and she was not symptomatic from urinary side she gave a history of bilharzizsis during childhood for which she received full treatment , patient had a successful renal transplant and was discharged with normal graft function on triple imuonsupression MMF Tacrolimus and Prednisolone, patient presented to emergency room with the complaint of dysurea and recurrent hematurea she mentioned that this symptoms is there for the last 6 months, investigations showed normal renal function, US showed urinary bladder adequately distended showing a large lobulated hyperechoic, hyper vascular mass without mobility measuring 4.6 x 3.3 x 6.2 cm corresponding to the volume of 51.6 ml along posterior and lateral walls. No stone is seen. MRI showed a large urinary bladder mass involving the posterior wall, both lateral walls and posterior superior wall. This mass exhibit low T2 signal intensity and shows diffusion restriction and enhancing post-contrast sequences. The mass does extend beyond the muscular layer . This mass is inseparable from the lower cervix and upper vagina suspicious for invasion. There is involvement vesicoureteric junction of the both sides causing grade IV left side hydroureteronephrosis. There is no synchronous mass seen within the ureter or the kidneys. The right transplant kidney shows grade II hydronephrosis and the ureter of the transplanted kidney is seen passing just anterior to the mass in the urinary bladder. . Cystoscopy and biopsy of the bladder mass and bladder wall showed Invasive keratinizing squamous cell carcinoma, moderately differentiated. Calcified ova of schistosoma species seen. patient has whole body CT scan which showed no metastasis Tc-99m HDP WB BONE SCINTIGRAPHY no scintigraphic evidences of bone metastasis Patient was taken to operation room and operated by a team from urology Ob Gyn and transplant ,anterior pelvic exentration(radical cystectomy,hystosalpingooverectomy,upper vaginectomy and most of the transplanted ureter she had ilieal conduit where its distal end was anastomosed to the pelvis of the transplanted kidney ( iliopyelostomy)and its proximal end fashioned as cutaneous stoma for urine drainage, patient was discharged with normal renal function and her latest creatinine is 73 umol/l
Conclusion: Cystoscopy and bladder biopsy must be included as a routine workup for any patient with history of bilharzizsis