Incidence of Viral Infections after Kidney Transplantation in a Single Pediatric Center
Majed Aloufi1, Abdulmonem Alghamdi1, Saeed Alghwery1, Saeed Alzahrani1, Naif Abdulmajeed1.
1Pediatric Nephrology, Prince Sultan Military Medical City, Riyadh, Saudi Arabia
Background: Viral infections are known threats after kidney Transplantation (KTx) causing significant numbers of mortality and morbidity.
Objective: To investigate the incidence of viral infections after KTx in children and the impact of controlled use of lower immunosuppression in allograft function.
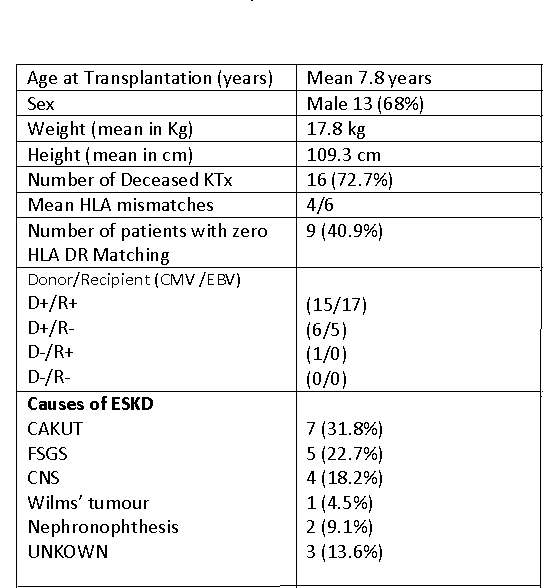
Methods: A review of children underwent KTx between 2010 and 2017. Baseline demographics, Immunosuppression agents, episodes of viral infections with Cytomegalovirus (CMV), BK Virus, and Epstein Barr Virus (EBV), and Serum Creatinine (SCr) were collected. All children received induction agents either Monoclonal or polyclonal antibodies, followed by Maintenance regimen (Tacrolimus & Mycophenolate mofetil (MMF) at 600mg/m2/day) with early steroids withdrawal. Oral valganciclovir is given to all high risk patients for 180 days as prophylaxis. CMV and EBV PCR are monitored every two weeks initially until the ninth month, then monthly until the end of the second year, and then every three months. Urine BKV PCR is monitored monthly in the first year, and then every three months.
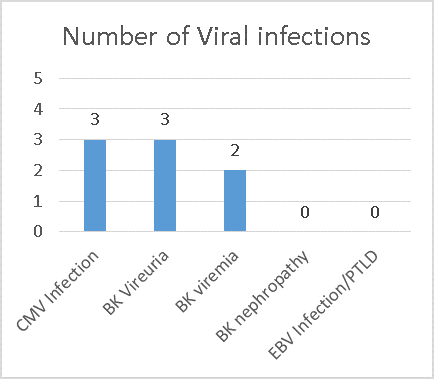
Results: A total of 22 children were transplanted. Three episodes of CMV infection (13.6 %) occurred with excellent response to treatment and secondary three months prophylaxis, three episodes (13.6%) of isolated BK Viruria, two of them with an episode of BK viremia (9.0%) with no associated BK nephropathy (0%) which responded to MMF dose reduction and oral Ciprofloxacin, no episodes of EBV or Lymphoproliferative Disease (PTLD) (0%). Allograft functions continued to be stable with mean SCr 54.3 umol/l during the study period with three episodes (13.6%) of acute cellular Rejection and one episode (4.5%) of early ABMR.
Conclusion: Viral infection risk might be minimized by prolonged CMV prophylaxis, as well as considering use of lower Mycophenolate dose and early steroids withdrawal, together with close viral monitoring protocol without compromising allograft function. Our study is limited by a retrospective design and a small sample size.