
Impact of Delayed Graft Function without Dialysis Needed
Carlos Arias-Cabrales1, María José Pérez-Sáez1, Dolores Redondo1, Carla Burballa1, Marisa Mir1, Marta Crespo1.
1Neprhology, Hospital del Mar, Barcelona, Spain
Introduction: Delayed graft function (DGF), defined as dialysis needed within the first week after transplantation are usually related with poor graft outcomes. There are few information about slow graft function without dialysis needed. For these reason, We aimed to study the impact of IGF vs SGF and DGF on renal function and graft survival both short and long-term, as well as the risk factors implicated on SGF/DGF development.
Material and Methods: Retrospective patient cohort based study from 589 five consecutive deceased donor kidney transplants (DDKT) in our center between January 2004 and December 2015. We excluded KT from donors younger than 18 years old (n=13) and all cases of primary non function (PNF). We evaluated graft survival and graft function at one and five years.
Results: 451 KT were included in the final analysis. DGF was developed in 187 (41.5%) recipients , 186 (41.2%) developed SGF and 78 presented IGF (17.3%). Univariate logistical regression analysis showed that donor’s age and gender, recipient’s age, time on dialysis, history of arterial hypertension and diabetes mellitus, and cold ischemia time (CIT), were related to DGF. KDPI was also related to SGF development. The adjusted analysis performed by multivariate logistical regression showed as independent risk factors to develop DGF: CIT (OR 1.076 [1.034-1.119]; p<0.001), donor gender (male) (OR 3.840 [1.059-2.469]; p=0.026), recipient’s history of arterial hypertension (OR 2.348 [1.391-3.964]; p=0.001), time on dialysis (OR (per month) 1.009 [1.001-1.017]; p=0.028) and age at the time of KT (OR (per year) 1.019 [1.003-1.035]; p=0.020). The analysis addressed to evaluate independent risk factors for SGF showed high risk in KT recipients from donors with higher KDPI score (OR (per point in KDPI) 1.010 [1.002-1.018]; p=0.018) and recipient with history of diabetes mellitus (OR 2.188 [1.404-3.410]; p=0.001).
We registered 85 graft losses during the follow-up; 46 death-censored graft losses and 39 patients who died with a functioning kidney. Four patients were lost to follow-up.
Univarite analysis both DGF and SGF were related with worse graft function 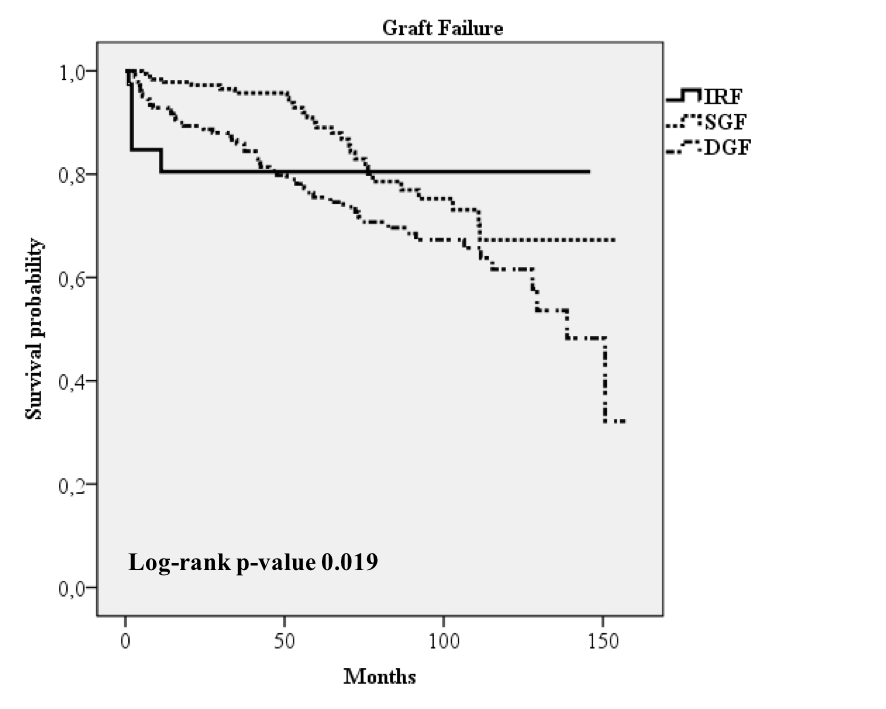 and graft renal function at 1 and 5 years.
and graft renal function at 1 and 5 years. 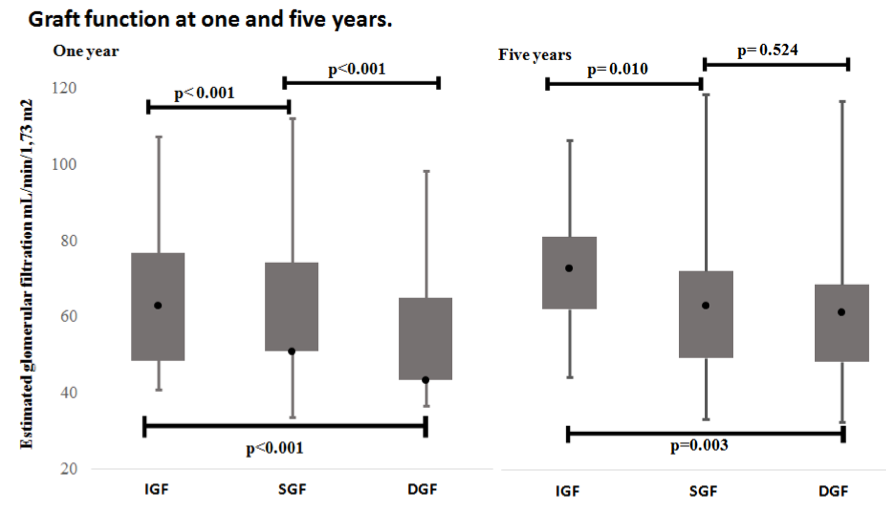 However in multivariate analysis neither DGF nor SGF are not related with graft outcomes and SGF was related with best graft survival (HR to graft loss 0.19 [0.06-0.65], p=0.008). According to graft function impact DGF and SGF were related with lower estimated glomerular filtration at one year (HR 1.94 [1.02-3.66; p=0.043]; HR 2.50 [1.12-5.61; p=0.026]). At 5 years only SGF was related with worse graft function (HR 4.27 [95%IC 1.18-15.47; p=0.027])
However in multivariate analysis neither DGF nor SGF are not related with graft outcomes and SGF was related with best graft survival (HR to graft loss 0.19 [0.06-0.65], p=0.008). According to graft function impact DGF and SGF were related with lower estimated glomerular filtration at one year (HR 1.94 [1.02-3.66; p=0.043]; HR 2.50 [1.12-5.61; p=0.026]). At 5 years only SGF was related with worse graft function (HR 4.27 [95%IC 1.18-15.47; p=0.027])
Conclusions: Several donor, recipient and transplantation variables are related with DGF and SGF. Classical definition of DGF as dialysis needed do not provide adequate graft prognostic information in our sample, additionally IGF could be a best form to define graft function recovery in terms of prognostic capacity.

