

Outcome of Robotic Assisted Laparoscopic Kidney Transplantation With and Without Regional Hypothermia
Pranjal Modi1, Bipin Chandra Pal1, Suresh Kumar1, Rohit Chauhan1, Vivek Kothari1, Amit Mishra1, Manisha Modi3, Veena Shah3, Vivek Kute2, Himanshu Patel2, Pankaj Shah2, Varsha Trivedi4, Hargovind Trivedi2,4.
1Transplantation Surgery and Urology, Institute of Kidney Diseases and Research Centre, Ahmedabad, India; 2Nephrology, Institute of Kidney Diseases and Research Centre, Ahmedabad, India; 3Transplant Anesthesia and Critical Care, Institute of Kidney Diseases and Research Centre, Ahmedabad, India; 4Immunology, Institute of Kidney Diseases and Research Centre, Ahmedabad, India
Introduction: During vascular anastomosis the kidney graft slowly gain temperature and becomes warm. Regional hypothermia is shown to be effective to reduce rewarming of the kidney during robotic assisted laparoscopic kidney transplantation (RKT). Currently there is no study available to compare impact of regional hypothermia versus no hypothermia during RKT. Here we present data of RKT with and without regional hypothermia.
Material and methods: RKT was carried out in 100 patients; the first 50 cases had regional hypothermia and later 50 cases did not have hypothermia. Regional hypothermia was created by introducing 250-300 ml of ice slush around the kidney before carrying out vascular anastomosis. Body surface warming was carried out in all cases of regional hypothermia. Living donor kidney with single renal artery and vein was used in all cases.
Results: No case was converted to open operation. Longer anastomosis time and operative time in initial 50 cases represents learning curve of RKT. 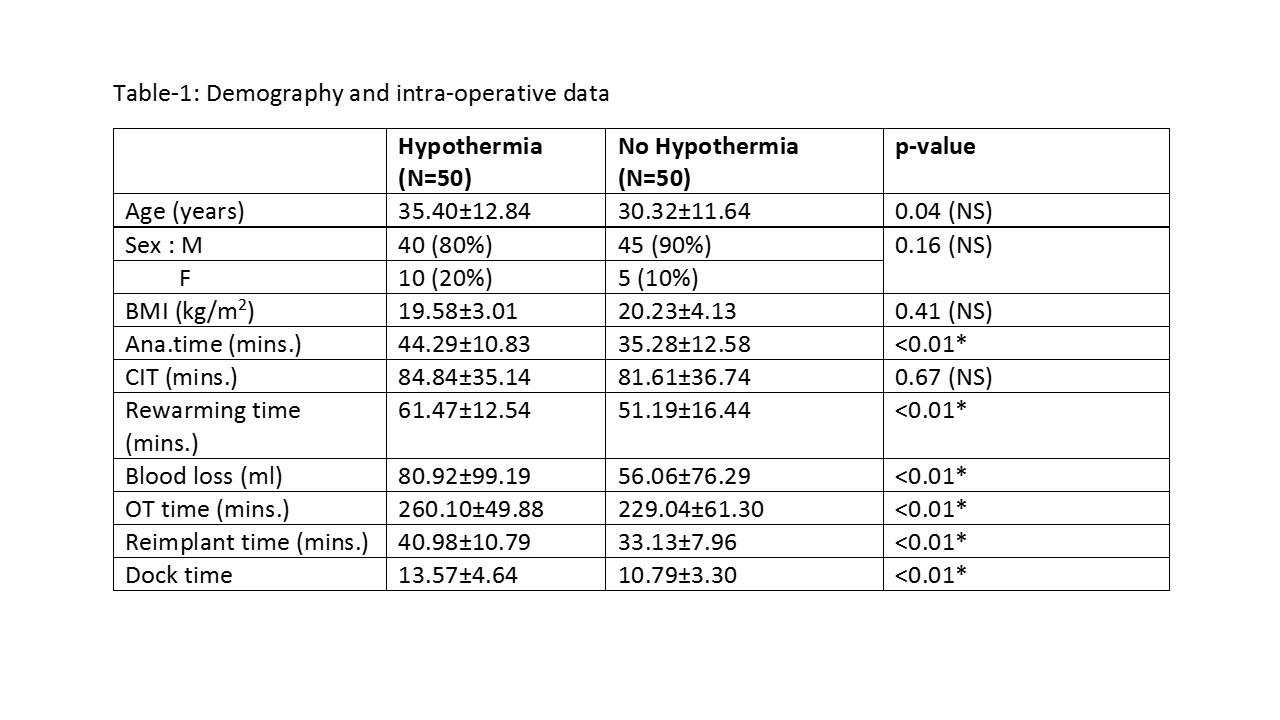 No delayed graft function was observed in any case and graft function was measured in terms of serum creatinine. (Figure-1)
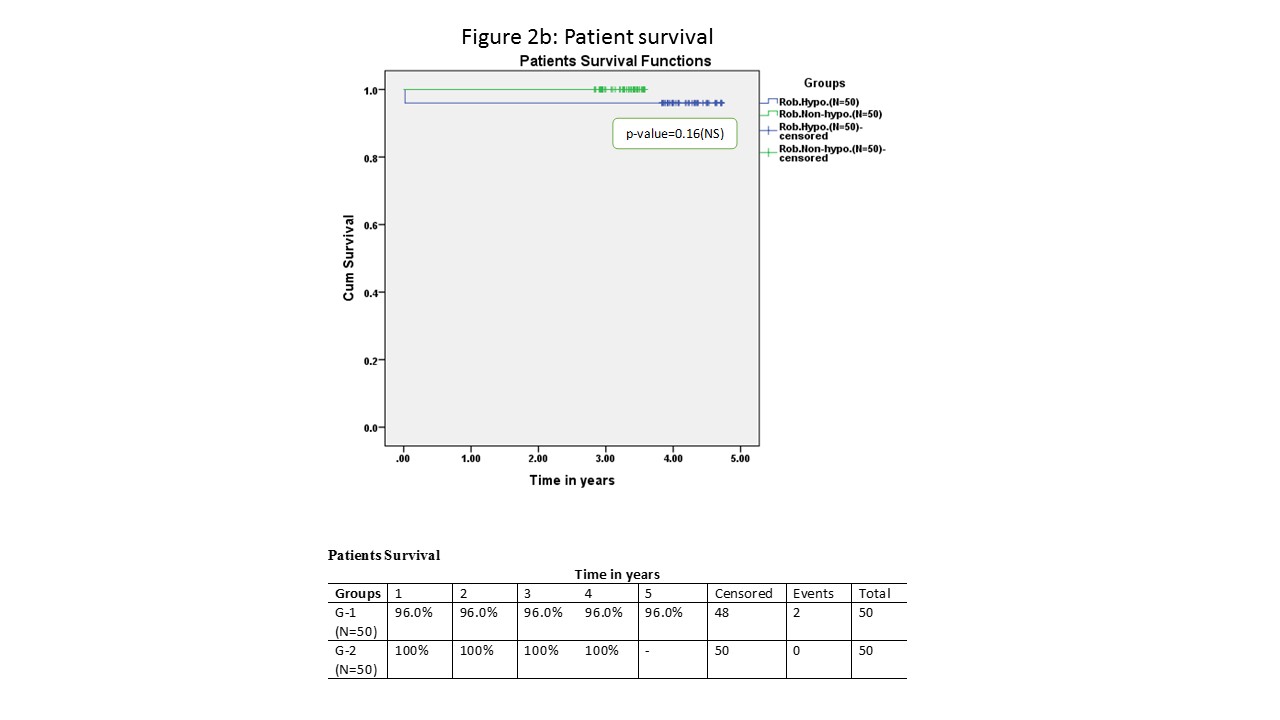
No delayed graft function was observed in any case and graft function was measured in terms of serum creatinine. (Figure-1)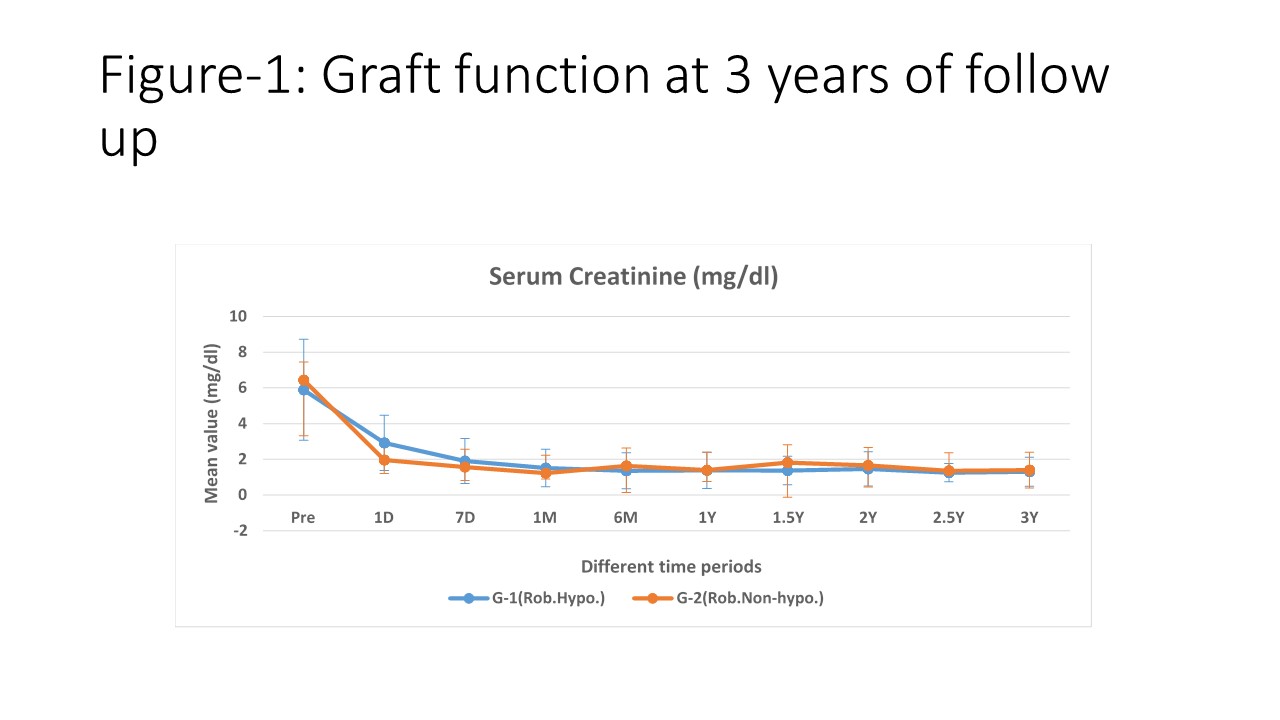 . At 3 years there was no difference in graft and patient survival in either group (Figure-2a and 2b)
. At 3 years there was no difference in graft and patient survival in either group (Figure-2a and 2b)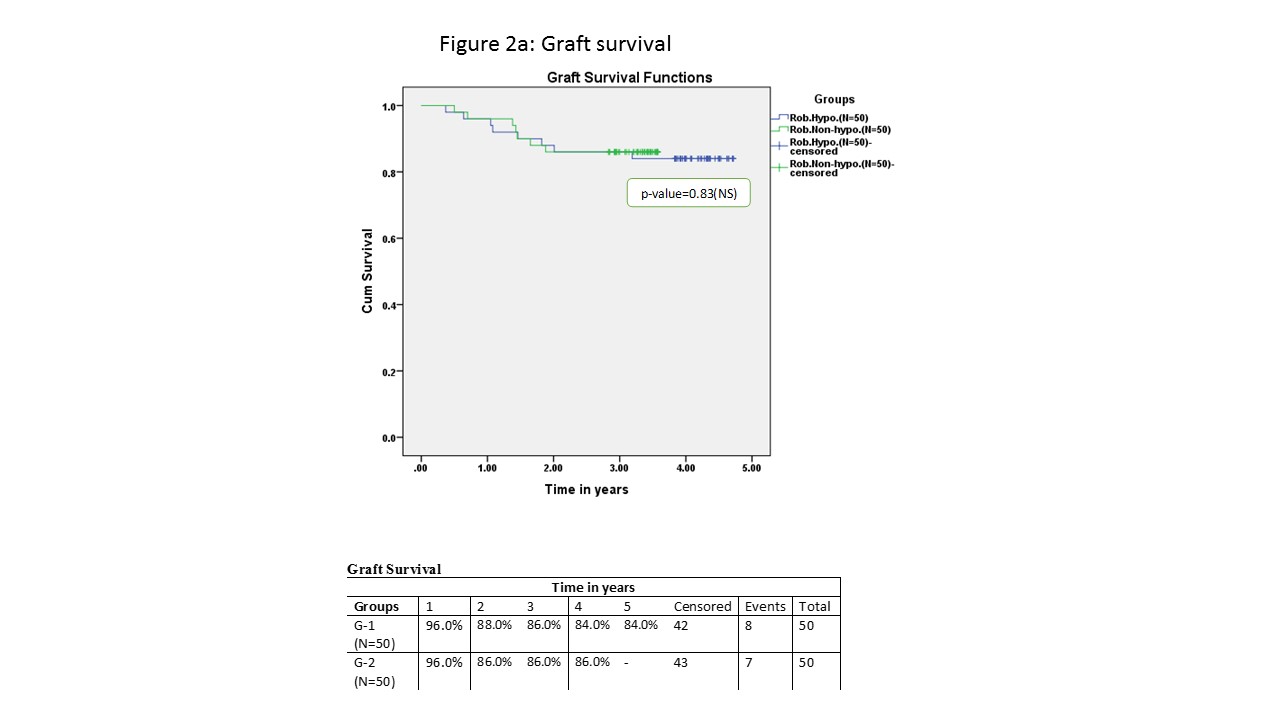
 Three patients in regional hypothermia group developed severe systemic hypothermia (temp. 94 degree F) and needed extubation in intensive care unit 6-12 hours after completion of surgery.
Three patients in regional hypothermia group developed severe systemic hypothermia (temp. 94 degree F) and needed extubation in intensive care unit 6-12 hours after completion of surgery.
Conclusion: Regional hypothermia using ice slush may be useful during learning of RKT; however, once anastomosis time is reduced to less than 40 minutes, outcome of RKT without reginal hypothermia are similar to RKT with regional hypothermia. Severe systemic hypothermia may occur and intra-operative warming is required in patients subjected to regional hypothermia.

